click for large version
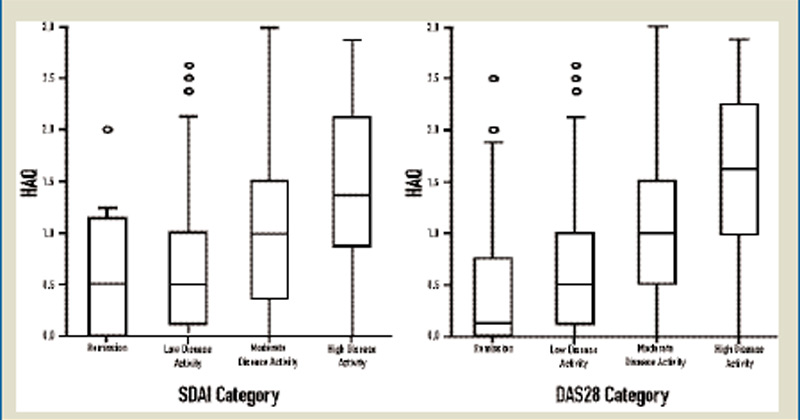
Figure 1: Relationship of categories of disease activity, as determined by the Simplified Disease Activity Index (SDAI) and the Disease Activity Score using 28 joints (DAS28), with physical function, as determined by the Health Assessment Questionnaire (HAQ), in 767 patients. For both the SDAI and the DAS28, P< 0.01, by Kruskal-Wallis H-test statistics (nonparametric analog of a one-way analysis of variance). Note the similarity of HAQ values when comparing the low, moderate, and high disease activity states of both SDAI and DAS28 but the differences in median values as well as upper quartiles when comparing remission states of the two scores. Source: Arthritis Rheum. 2005;52:2625-2636.
click for large version
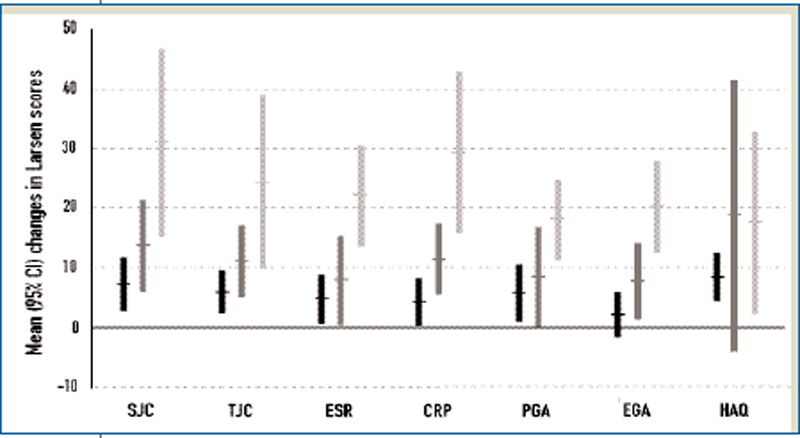
Figure 2: Relation of ratings by rheumatologists to outcome. Mean and 95% confidence intervals (CIs) for changes in Larsen scores over the three-year observation period in 65 patients in an inception cohort are shown for patients who spent most the time (i.e., >18 months) in remission (black error bars), low disease activity (dark grey error bars), or moderate and high disease activity (light grey error bars), separately for the seven core-set measures. The associations with disease activity and Larsen were highly significant (P<0.001). Note that lowest progression of radiographic damage was seen for longitudinal remission, not longitudinal low disease activity. ESR, 0–100 mm; CRP, 0–100 mg/l; PGA and EGA, 0–100 mm; HAQ, 0–3.
Source: Rheumatology. 2006;45:1133-1139.
Source: Rheumatology. 2006;45:1133-1139.
When one strives for remission, one is aiming to achieve a disease a state (or disease activity category) rather than a mere proportional improvement. This means that patients with high disease activity have to experience larger changes than patients with moderate or low disease activity. Remission is associated with a much smaller reduction of inflammatory load in patients with moderate disease activity than patients with high disease activity. Striving for remission requires rethinking our attitude toward therapeutic goals and standards.
But how do we best measure remission?
