 CHICAGO—Temporal artery biopsy (TAB) has long been the gold standard for the diagnosis of giant cell arteritis (GCA). However, with continued advancements in ultrasound resolution and growing provider expertise, temporal artery ultrasound (TAUS) is increasingly being used in practice. This shift is reflected in the differing recommendations of the ACR/VF and EULAR guidelines, with the European guidelines now favoring ultrasound as the initial imaging modality.1,2 In the ACR Convergence 2025 session, Great Debate: Ultrasound vs. Temporal Artery Biopsy in Giant Cell Arteritis, two vasculitis experts went head to head to determine the ideal first test in the diagnosis GCA.
CHICAGO—Temporal artery biopsy (TAB) has long been the gold standard for the diagnosis of giant cell arteritis (GCA). However, with continued advancements in ultrasound resolution and growing provider expertise, temporal artery ultrasound (TAUS) is increasingly being used in practice. This shift is reflected in the differing recommendations of the ACR/VF and EULAR guidelines, with the European guidelines now favoring ultrasound as the initial imaging modality.1,2 In the ACR Convergence 2025 session, Great Debate: Ultrasound vs. Temporal Artery Biopsy in Giant Cell Arteritis, two vasculitis experts went head to head to determine the ideal first test in the diagnosis GCA.
Ultrasound Should Replace Biopsy for GCA Diagnosis
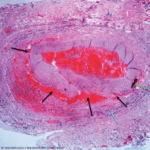
As the first person to describe the ultrasound halo sign in GCA, Wolfgang Schmidt, MD, MACR, Professor of Charité University Medicine at Waldfriede Hospital, Berlin, was well suited to argue his position. He also pioneered the GCA fast-track clinic. Accordingly, he opened his presentation by making it clear he felt strongly about encouraging clinicians to start with ultrasound when diagnosing GCA.

Dr. Wolfgang Schmidt
Dr. Schmidt made note of the change in practice patterns over the past two decades, with providers moving from TAB to TAUS. In the updated EULAR guidelines for large-vessel imaging, TAUS is recommended as the first-line modality for GCA diagnosis.2
Using the ACR/EULAR classification criteria for GCA, he demonstrated that ultrasound has greater potential diagnostic yield. Although both positive TAB and TAUS represent five points on the criteria, confirmation of bilateral axillary involvement with ultrasound provides an additional two points toward the diagnosis.3