How to Avoid Lawsuits
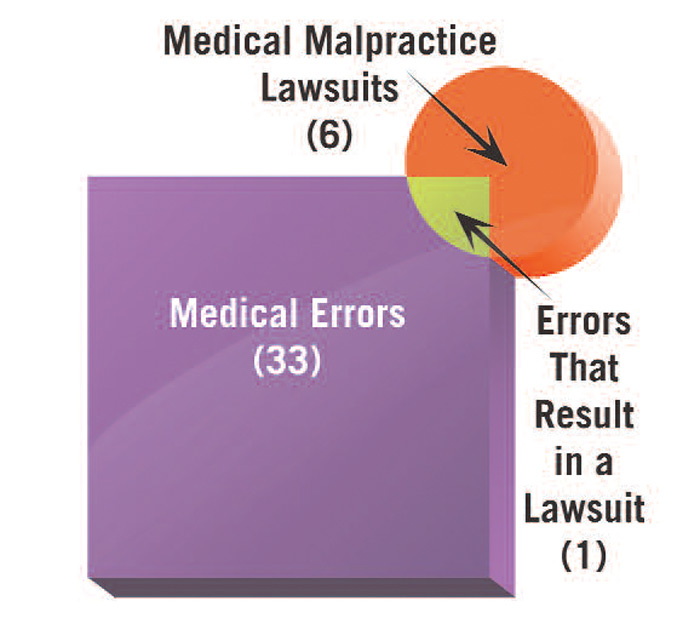
The classic paper on malpractice by Brennan and colleagues stated that only one of six lawsuits has a medical error at its core.5 (See Figure 1) If not for medical errors, then why are physicians sued? Research suggests that reasons for suits include patient dissatisfaction with the physician’s communication skills, trying to obtain more information about their care, concern about a cover-up, and desire for remuneration.6
The first and foremost risk-management tool is a good doctor–patient relationship.7 If patients like you and they feel you were negligent, they consider it a mistake. Everyone makes mistakes. Doctors are forgiven. If they don’t like you and they feel you’re negligent, then they consider it malpractice.8 We all know of physicians who deliver poor care, yet their patients never sue because of their positive feelings toward the doctors. One needs to be alert when caring for high-risk patients (either angry or sick) – especially those who have chest, neurological, or infectious symptoms (heads, hearts, and bugs).