The modified criteria can be used to diagnose most patients, including a large percentage of the 20% to 60% of children who develop aneurysms but never meet KD criteria. Further work is needed to develop criteria to identify patients at risk for these aneurysms and tailor therapy accordingly. He emphasized that many cases of KD include unusual features such as shock physiology or acute abdominal symptoms. Among the most helpful information for clinicians trying to diagnose KD is to recognize certain findings that are seldom seen in KD (see Table 2).
Treatment Options
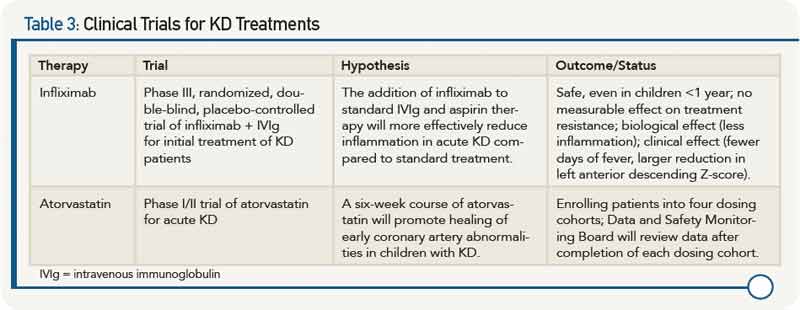
Dr. Burns reviewed clinical trial data on new treatments for KD (see Table 3).
Based on the data, she said that infliximab should be considered in children with high inflammation and those with early coronary artery changes. “A single dose of infliximab (5 mg/kg) is safe and well tolerated in patients with acute Kawasaki disease and reduces fever, inflammation, and coronary artery internal diameter faster,” she said.
Although data on atorvastatin is still pending, Dr. Burns emphasized that statins may hold promise for mitigating coronary artery damage in the acute phase.
She also presented data from the San Diego Adult KD Collaborative study that is beginning to address the future of KD patients and cardiovascular health by looking at the effect of KD on future cardiovascular health, the risk (if any) for people with normal echocardiograms during acute illness, and the feasibility of stratifying patients based on risk using simple, noninvasive tests. Results of one study published in 2012 that looked at computed tomography (CT) calcium scores in KD patients years after KD diagnosis found no calcification in patients with a history of KD and normal coronary arteries during the acute phase of the disease, and found that coronary calcification, which may be severe, occurs late in patients with coronary aneurysms.3 These results suggest, according to Dr. Burns, the usefulness of CT calcium scoring to screen patients with a remote history of KD or suspected KD and unknown coronary artery status.