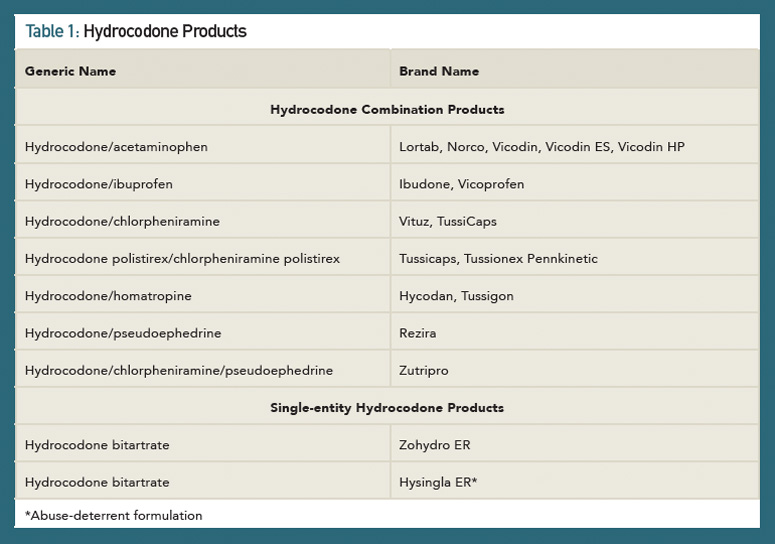
In 2012, the FDA approved a risk evaluation and mitigation strategy (REMS) for highly potent opioids, such as extended-release (ER) and long-acting (LA) medications.7,8 A major goal of opioid REMS programs was to reduce harm from prescription opioid misuse and abuse while continuing to provide access to these medications for patients’ pain management. Another strategy to achieve the goal of reducing harm from opioids was the development of abuse-deterrent formulations. Abuse-deterrent formulations are designed to reduce people’s ability to extract the active opioid ingredient from the dosage form. Individuals can try to do this by chewing the formulations and/or smashing them into a powder so they snort or inject the opioid. In late November (2014), the FDA approved hydrocodone bitartrate (Hysingla ER) as an “abuse-deterrent” tablet that cannot be easily crushed or chewed.9 The product forms a thick gel when crushed, making it difficult to inject. At the time of this writing, Table 1 lists the currently available HCPs and single-entity hydrocodone products.


