click for large version
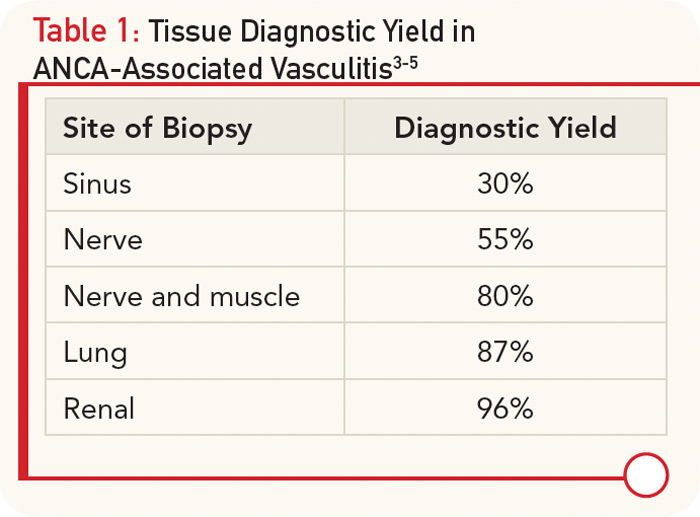
Table 1: Tissue Diagnostic Yield in ANCA-Associated Vasculitis3-5
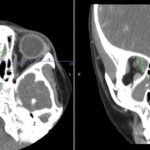
RB’s presentation, while in many ways classic for GPA, also had some atypical features. Specifically, genitourinary involvement is an uncommon presenting symptom in AAV, with only case reports describing prostatic, urethral, and penile involvement.6,7 However, an autopsy series done over 50 years ago demonstrated prostatic involvement in 7% of patients with GPA.8 Despite widespread systemic disease, he lacked any significant musculoskeletal symptoms, fevers, or rash. It has been reported that fewer than 70% of patients have prominent musculoskeletal complaints and less than a quarter of patients have skin disease at presentation.1,5