Case Summary
A 55-year-old woman presented at our facility with complaints of shortness of breath and swelling of her face, throat, hands and feet. Her past medical history included ulcerative colitis with no flare despite a decade off of all medications. She had hypertension and hypothyroidism, which were well controlled on levothyroxine. The surgical and family history were non-contributory. Her social history was significant for years of exposure to a wood-stripping agent.
The patient believed her illness had begun eight months earlier when she first presented to her primary care provider with several, non-painful, enlarged cervical lymph nodes, odynophagia, fatigue and, later, generalized body swelling.
The outpatient workup was unrevealing, and before a lymph node biopsy could be performed, repeat imaging demonstrated resolution of the patient’s lymphadenopathy. During the primary care workup, she was treated with diuretics, as well as prednisone, without symptomatic improvement, and she had stopped these medications prior to presentation at our facility.

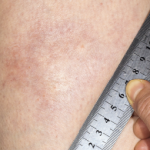
Figure 1. Evidence of the patient’s small oral aperture at the time of presentation.

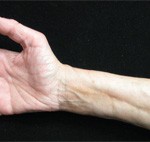
Figure 2. The prayer sign, which is rarely seen in patients suffering from eosinophilic fasciitis.