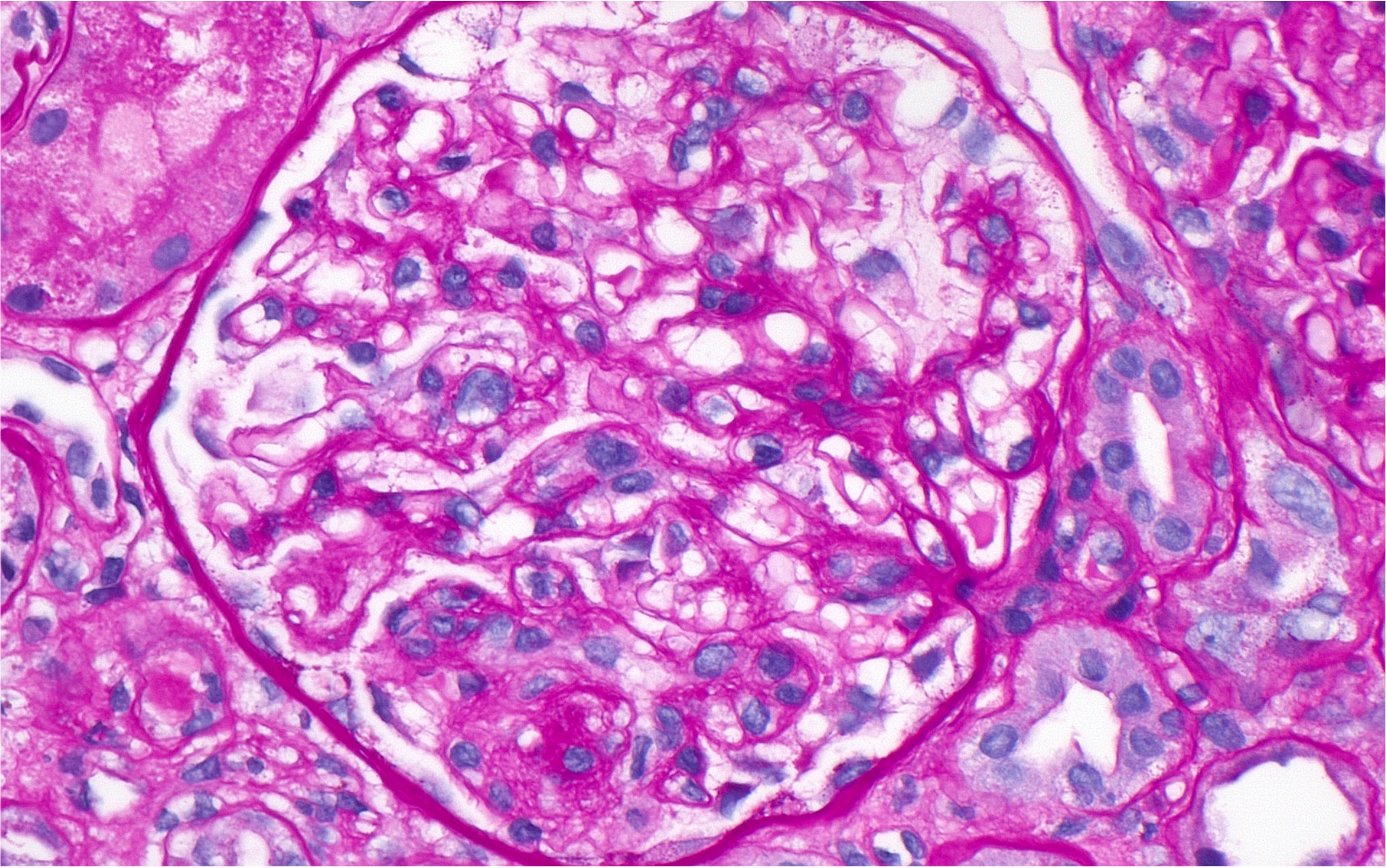
Figure 4: Glomerulus showing FSGS. (Click to enlarge.)
After the first dose of rituximab, the patient was noted to have a stable renal response, with an eGFR of 44 mL/min/1.73 m2, creatinine of 1.30 mg/dL and urine protein to creatinine ratio of 469 mg/g.
Discussion
Lupus podocytopathy clinically presents as nephrotic range proteinuria, which correlates with the extent of foot process effacement.3,6 The diagnostic criteria proposed by Hu et al. are:2