
SNOWMASS, COLO.—Testing for antibodies to neutrophil cytoplasmic antigens (ANCA) can be clinically useful, but test results sometimes require further investigation, according to Ulrich Specks, MD, professor of medicine at the Mayo Clinic College of Medicine and chair of the division of pulmonary and critical care medicine at the Mayo Clinic in Rochester, Minn. “There is no perfect ANCA test. That is one truth that everyone needs to walk away with,” Dr. Specks said during a session titled, “Clinical Utility of ANCA Testing,” here at the ACR Winter Rheumatology Symposium, held January 26–February 1, 2013. “Not even a perfect test could give you a definitive answer to all clinical questions.”
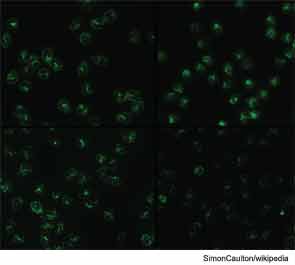
Various testing methods are used to identify types of ANCA with different specificities. Immunofluorescence microscopy is used to identify two major categories of ANCA—with cytoplasmic staining (C-ANCA) or with artifactual perinuclear staining (P-ANCA)—and these can have specificity for proteinase 3 (PR3) and myeloperoxidase (MPO). The most frequently used tests for antigen-specific detection are enzyme-linked immunosorbent assay (ELISA) methods, Dr. Specks said. These include direct ELISA and capture ELISA. With direct ELISA, there is always a tradeoff of analytical sensitivity versus specificity, he added, saying this is especially true with PR3, which is difficult to purify. Capture ELISA, on the other hand, is designed to get around the issue of specificity, but has the potential of a false negative because of competition for antigens in the target assay.

