click for large version
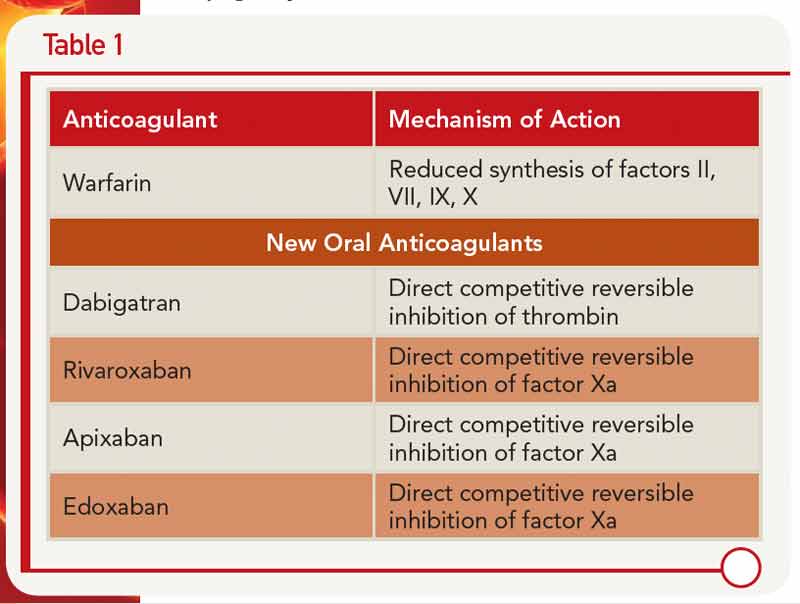
Table 1
click for large version
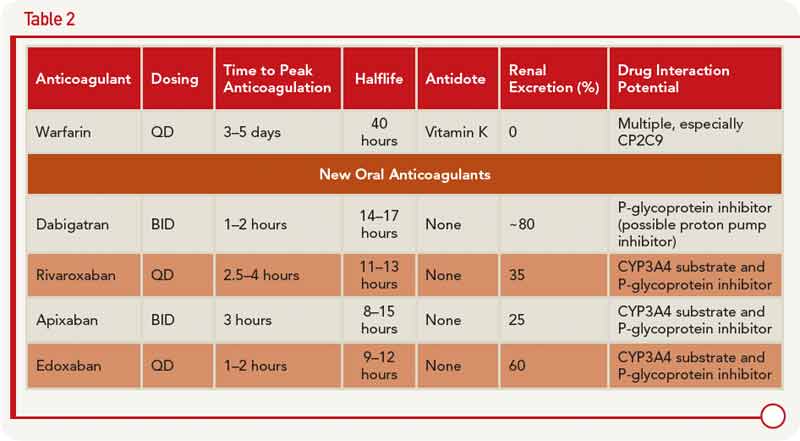
Table 2
New Anticoagulants: Pros and Cons
Dr. Kessler described the pharmacology of the new oral anticoagulants along with warfarin, including the different mechanisms of action (see Table 1) and clinical application (see Table 2).
A number of advantages and disadvantages should be weighed when considering use of one of these new anticoagulants over warfarin, he said. The advantages include lower rates of stroke and mortality, along with lower rates of intracerebral hemorrhage (although the rates of gastrointestingal bleeding are higher) compared to warfarin. One of the main advantages, he said, is that these anticoagulants are more convenient to use because they don’t require the type of regular monitoring that warfarin requires.


