New Paradigm of Coagulation
Dr. Kessler laid the foundation for understanding the role for the new oral anticoagulants by describing a new paradigm of coagulation that helps explain how rheumatological diseases trigger coagulation. In the older paradigm, described as a coagulation cascade, the thought was that tissue damage to the extrinsic circulating tissue factor and clotting factor VIIA complex activates the intrinsic pathway factor IX to initiate generation of thrombin for fibrinogen cleavage and fibrin formation.
According to Dr. Kessler, in the new paradigm, described as normal hemostasis, tissue-factor bearing cells are the mainstay of coagulation in which the process of FVIIa-tissue factor complex formation occurs on the surface of tissue factor laden cells, such as monocytes and macrophages. “These cells are critical to the symptomatology and progression of autoimmune diseases and links inflammation with coagulation,” he said, adding that new treatment strategies can be developed based on this new understanding of how rheumatological diseases trigger coagulation.
New Anticoagulants: Pros and Cons
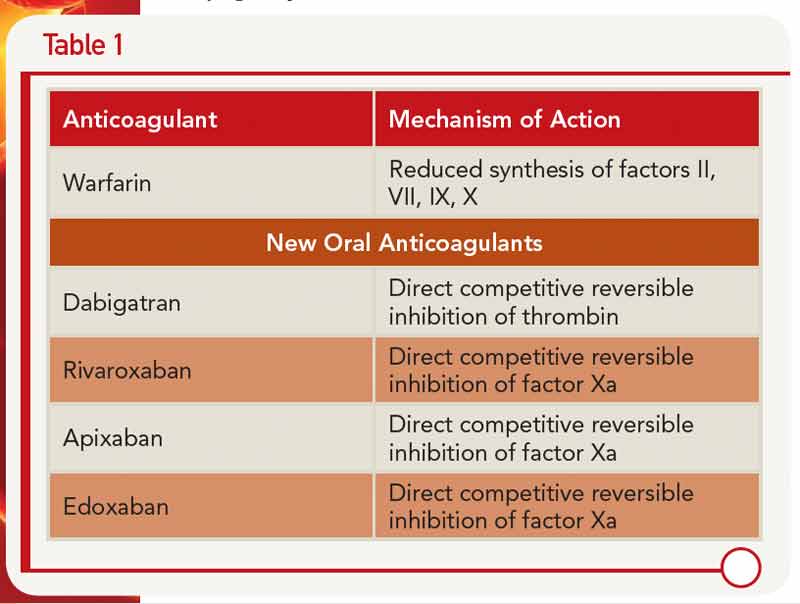
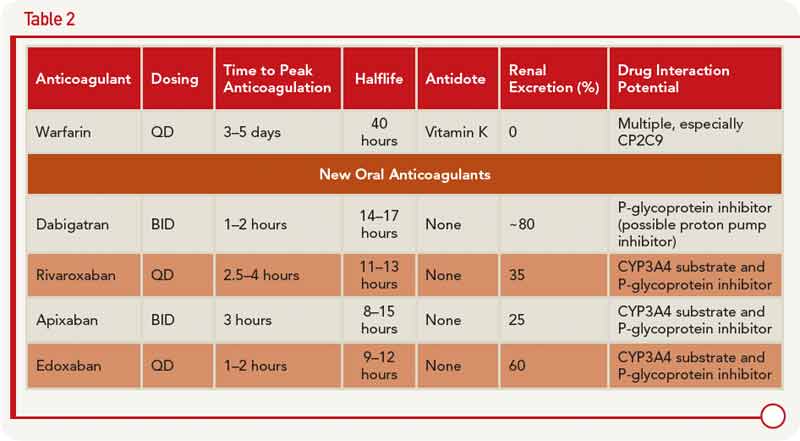
Dr. Kessler described the pharmacology of the new oral anticoagulants along with warfarin, including the different mechanisms of action (see Table 1) and clinical application (see Table 2).
A number of advantages and disadvantages should be weighed when considering use of one of these new anticoagulants over warfarin, he said. The advantages include lower rates of stroke and mortality, along with lower rates of intracerebral hemorrhage (although the rates of gastrointestingal bleeding are higher) compared to warfarin. One of the main advantages, he said, is that these anticoagulants are more convenient to use because they don’t require the type of regular monitoring that warfarin requires.
However, the lack of monitoring could also affect adherence adversely, he said. Other disadvantages of the new anticoagulants include the short half-life, which may not benefit patients with limited adherence, as well as the inability to titrate doses and the high cost of these drugs. One main disadvantage, he said, is that these new anticoagulants have no antidote. To address this, he cited a study by Kaatz et al. that provides some information and suggestions on reversal of three of the new anticoagulants, apixaban, dabigatran, and rivaroxaban.1 For example, oral activated charcoal can be used to reverse all three of these anticoagulants, whereas fresh frozen plasma will not be effective for any of these.
Mary Beth Nierengarten is a freelance medical journalist based in St. Paul, Minn.


