Bottom line: We need to not only improve how often we measure, but how we measure disease activity to make optimal treatment decisions, especially considering the recently described consequences of failing to control active disease.11
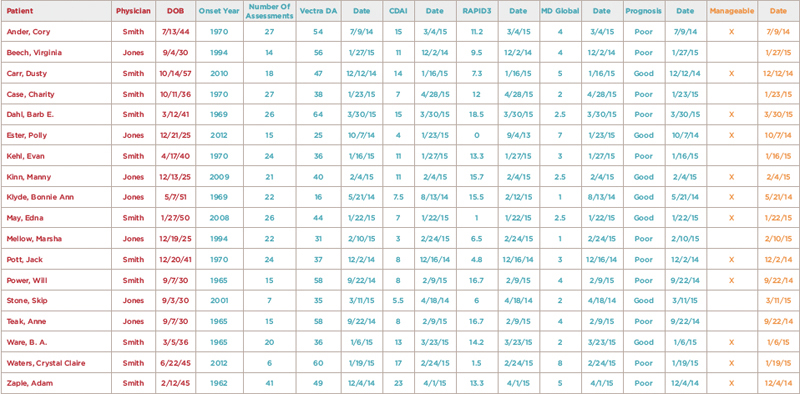
(click for larger image) Figure 1: Example Disease Registry Spreadsheet
Note: This spreadsheet includes patient and managing physician identifiers (red), information critical for disease management (teal), and whether each patient’s disease can be managed or not (orange). Each column can be sorted to stratify disease duration, disease activity, last assessment dates (on time and overdue), prognosis and manageability (yes or no). An individual patient’s accumulated assessments can be viewed separately and tracked to facilitate their individual treatments in most available disease registries.
Confront the Problems
Here’s what RAPP physicians are doing differently to address these critical practice problems: