Designua / shutterstock.com
SAN DIEGO—Treatments do exist that can improve the prospects of a patient with the rare disease amyloidosis, but only if clinicians keep the disease in mind and treat the patient before it’s too late, an expert said at the 2017 ACR/ARHP Annual Meeting this past November. He also discussed research that may be close to verifying a new drug treatment for the devastating disease.
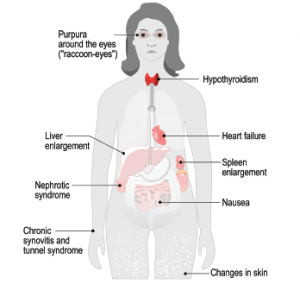
“The first and most important thing I want to say to you is, think amyloidosis,” said Sir Mark Pepys, MD, PhD, professor of medicine at University College London in England. Dr. Pepys has been studying amyloidosis for decades, and he founded the UK National Amyloidosis Center, also in London. “Please remember to think amyloidosis when you’re confronted with any clinical case at all. Systemic amyloidosis can mimic just about any clinical presentation you want to talk about, and if you don’t think of it, you’re not going to do the right diagnostic investigations. If you don’t make the diagnosis, the patient will suffer.”