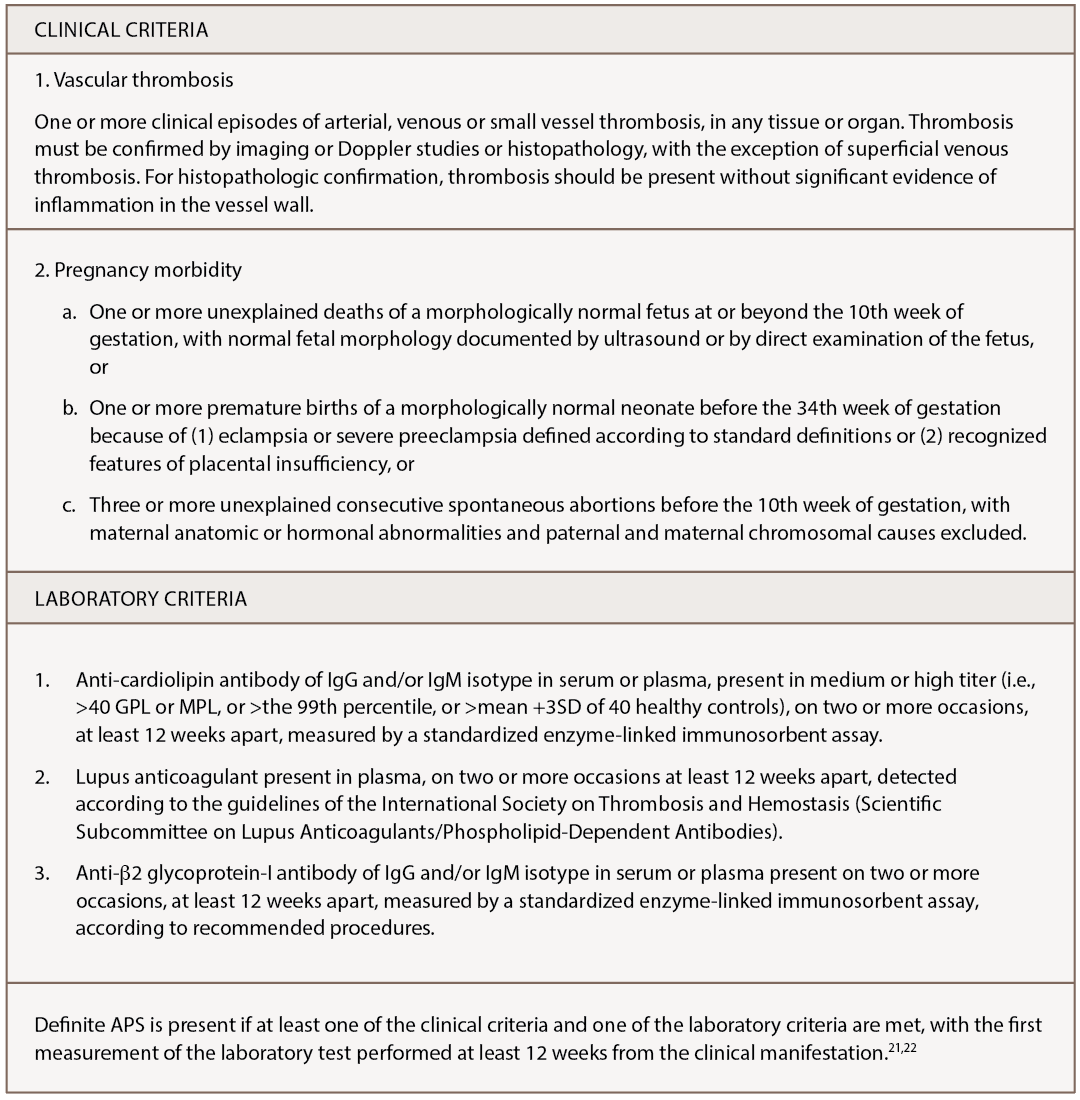
(click for larger image) Table 1: Classification of Antiphospholipid Syndrome
Of note, however, not every positive antiphospholipid antibody (aPLA) is clinically significant, and not every patient with positive aPLA has the same risk. Other factors, such as cardiovascular disease and recent trauma, play a role. A clinically significant anti-cardiolipin antibody greater than or equal to 40 units or anti-β2 glycoprotein-I antibody greater than or equal to 40 units is tested twice at least 12 weeks apart.23 Further, a positive lupus anticoagulant test is based on guidelines from the International Society of Thrombosis and Haemostasis.21
Buddha Basnyat, MD, and colleagues describe a young man with APS who experienced vision changes and abdominal pain while climbing at 7,000 meters in the Himalayas.24 The patient was found to have superior mesenteric vein thrombosis, as well as multiple venous sinus thromboses.
