In the LONFLIT3 study, three high-risk groups were studied: One was given no prophylaxis, one was given ASA, and the last received low-molecular-weight heparin (LMWH; enoxaparin).27 Results revealed the group given enoxaparin developed no DVT, whereas several individuals in the other two groups did develop DVT. Several years later, the American College of Chest Physicians (ACCP) devised recommendations for those considered at high risk of VTE, which includes individuals with APS (see Table 2).28 In addition to recommending general measures for those at a low risk of clotting (e.g., minimize constrictive clothing, maximize hydration and carry out frequent calf muscle exercises [Grade 1C]), the ACCP suggests below-the-knee graduated compression stockings (Grade 2C) or a single dose of LMWH prior to flight (Grade 2C). It does not support the use of ASA for VTE prophylaxis (Grade 1B).28
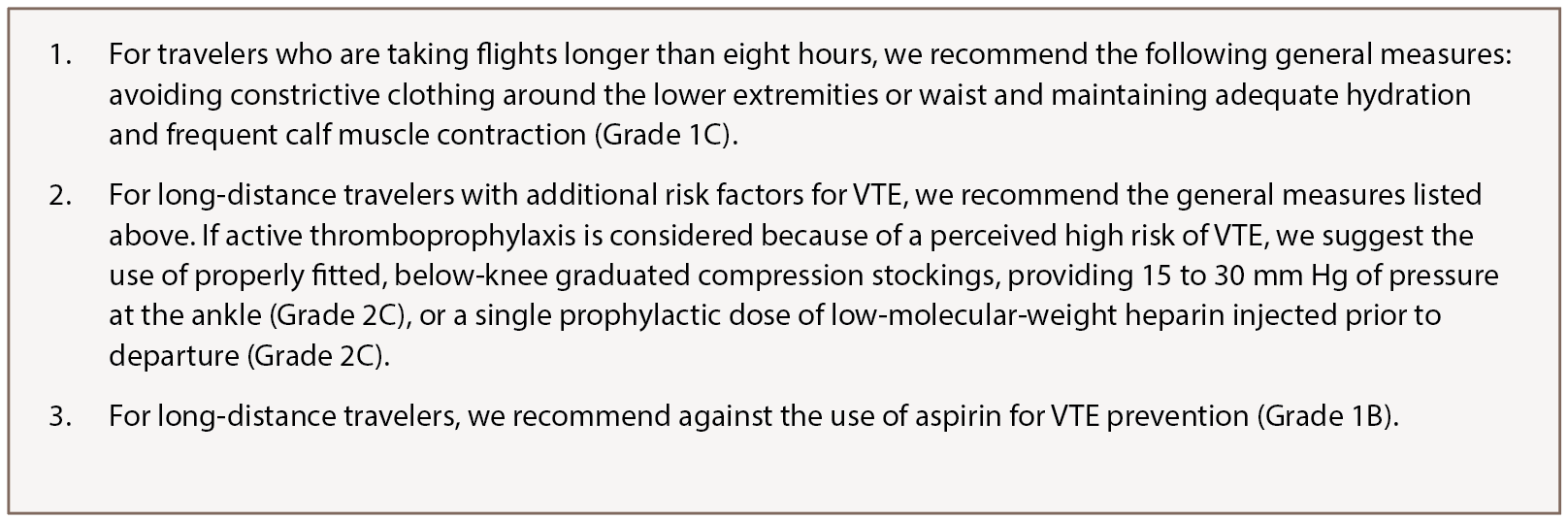
(click for larger image) Table 2: American College of Chest Physicians Long-Distance Travel Recommendations28
Authors’ Conclusions & Recommendations
It is prudent for practitioners to consider anticoagulation for high-risk patients with APS who are traveling for long distances or at high altitudes. When deciding whether to anticoagulate a patient positive for aPLA, it is important to be attentive of clinically significant laboratory values, as well as comorbidities associated with a greater increase in the risk of clotting. Further, in individuals with known APS, consideration for a booster dose of enoxaparin (1 mg/kg) is not unreasonable two to four hours prior to travel on flights exceeding eight hours’ duration. Although our recommendations are based on a review of the literature, further research is encouraged for patients with APS to assist in preventive measures and overall improved quality of life.
