 When coding evaluation and management (E/M) services provided to a patient, one of the most persistent concerns is whether a patient is new or established to the practice. Although this may seem like a simple coding answer, the distinction is an important one, because it enables providers to appropriately bill and receive reimbursement correctly. E/M service is a key factor in rheumatology practices and it is imperative that your coding hold up to any claims review to prevent payment delays.
When coding evaluation and management (E/M) services provided to a patient, one of the most persistent concerns is whether a patient is new or established to the practice. Although this may seem like a simple coding answer, the distinction is an important one, because it enables providers to appropriately bill and receive reimbursement correctly. E/M service is a key factor in rheumatology practices and it is imperative that your coding hold up to any claims review to prevent payment delays.
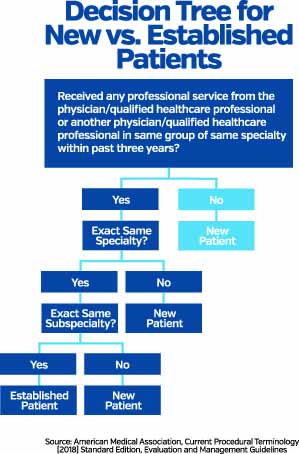
In 2012, the Current Procedural Terminology (CPT) manual made subtle changes to the definition of a new patient; unfortunately, the Centers for Medicare & Medicaid Services (CMS) did not change its definition to stay aligned with these updates. This discrepancy, along with the complex rules and regulations of E/M, has caused great confusion for many providers and their compliance efforts.

