| SLE Related | Non-SLE Related |
|---|---|
| Lupus enteritis | Appendicitis |
| Pancreatitis | Lithiasic cholecystitis |
| Pseudo-obstruction | Peptic ulcer |
| Acalculous cholecystitis | Acute pancreatitis |
| Mesenteric thrombosis | Retroperitoneal hematoma |
| Hepatic thrombosis | Ovarian pathology |
| Medications (NSAIDs, MMF, steroids, HCQ …) | Diverticulitis |
| Colon perforation (vasculitis) | Adhesions, intestinal occlusion |
| Infectious enteritis | |
| Pyelonephritis | |
| CMV colitis |
Key: NSAIDs: non-steroidal anti-inflammatory drugs; MMF: mycophenolate mofetil; HCQ: hydroxychloroquine.
Table 2: Anatomic Distribution of GI Involvement among Patients with SLE2
| Organ | Involvement |
|---|---|
| Mouth/pharynx | Oral ulcers |
| Esophagus | Dysphagia Esophageal dysmotility Gastric reflux Bullous epidermolysis Ulcerative esophagitis |
| Stomach | Peptic ulcer disease Gastric enteritis Dyspepsia |
| Pancreas | Acute pancreatitis |
| Liver | Hepatomegaly Type 1 autoimmune hepatitis Steatosis Nodular regenerative hyperplasia |
| Gallbladder | Primary sclerosing cholangitis Autoimmune cholangiopathy Acute acalculous cholangitis |
| Small Intestine | Celiac disease Mesenteric vasculitis Protein-losing enteropathy Cytomegalovirus enteritis Intestinal pseudo-obstruction |
| Colon | Crohn’s disease Bowel perforation Pneumatosis cystoides intestinalis Benign pneumoperitoneum |
| Rectum, anus | Ulcerations |
| Other | Appendicitis Primary lupus peritonitis Splenomegaly Ascites |
Lupus Enteritis
According to the BILAG 2004 definition, lupus enteritis is either vasculitis or inflammation of the small bowel with supportive imaging and/or biopsy findings.4 It may also be called mesenteric arteritis, intestinal vasculitis, enteric vasculitis, mesenteric vasculitis, lupus peritonitis or abdominal serositis.
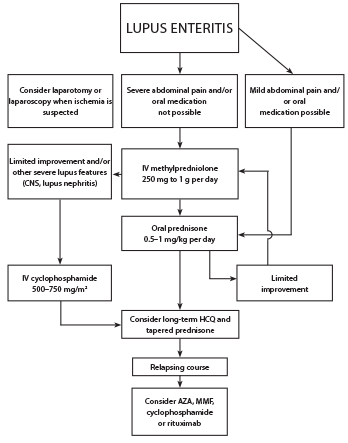
Figure 4: Proposed Treatment Algorithm for SLE Patients with Lupus Enteritis3
Although the pathogenesis of lupus enteritis remains unknown, it has been reported that immune complex-mediated visceral vasculitis may result in bowel wall and mucosal edema.5 The most common clinical manifestations include abdominal pain, ascites, nausea, vomiting, diarrhea and fever (see Figure 3,).3
Lab findings in lupus enteritis include anemia (52%), leukocytopenia and/or lymphocytopenia (40%), thrombocytopenia (21%) and hypocomplementemia (88%).3

