Click to enlarge.
The clinical criteria include one or more episodes of venous, arterial or small vessel thrombosis within any tissue or organ confirmed with unequivocal imaging or histopathology. The second clinical criterion is pregnancy morbidity, with three subsets of situations included. The first is the occurrence of one or more unexplained deaths of a morphologically normal fetus at or beyond the 10th week of gestation. Normality of the fetus must be confirmed by ultrasound or direct examination. The second includes one or more premature births of a normal neonate before the 34th week of gestation. This premature birth can be due to severe preeclampsia, eclampsia or placental insufficiency. The third is three or more unexplained, consecutive, spontaneous abortions before the 10th week of gestation.
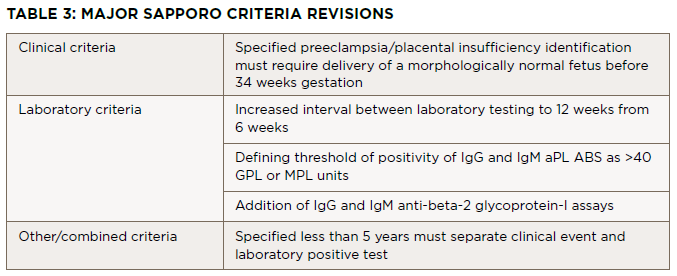
Three laboratory criteria exist. First is the presence of lupus anticoagulant in plasma on two or more occasions at least 12 weeks apart. The second and third criteria are the presence of anti-cardiolipin and beta-2 glycoprotein-I antibodies respectively, (IgG or IgM isotypes) on two or more occasions at least 12 weeks apart. Miyakis et al. discussed the inclusion of skin manifestations such as livedo reticularis as independent criteria for diagnosis, but due to a lack of specificity this was rejected.2 Digital gangrene did not merit inclusion because it was considered rare.2
