
Master1305 / shutterstock.com
We report on a 77-year-old patient who was diagnosed with giant cell arteritis (GCA) on histopathology of the submandibular gland and eventually went on to develop classic signs and symptoms of GCA. This observation highlights neck swelling as a rare initial presentation of GCA.
Case Presentation
A 77-year-old previously healthy man presented to his primary care physician with painless left-sided neck swelling of six months’ duration. Magnetic resonance imaging of the neck demonstrated diffuse homogenous enhancement of the left submandibular gland.
Given the submandibular gland findings, prednisone was recommended for treatment of focal GCA; however, the patient declined treatment and instead remained under close clinical observation with his rheumatologist.
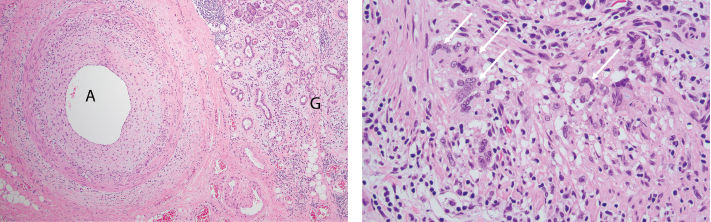
FigureS 1A (left) & 1B: Pathologic Findings of Submandibular Gland Resection
1A) A low-power photomicrograph demonstrates active giant cell arteritis with intimal proliferation and medial chronic inflammation consisting of lymphocytes, macrophages and occasional giant cells within a small artery (A). Chronic sialadenitis manifests as chronic inflammation, fibrosis and gland dropout in the glandular tissue (G). H&E stained section, 40x original magnification.
1B) A high-power photomicrograph demonstrates numerous giant cells (arrows) within the arterial wall. H&E stained section, 200x original magnification.
Eight months later, he developed pain in the right temple, as well as jaw pain with chewing. His ESR and CRP were elevated at 46 mm/hr and 41 mg/L, respectively. Vascular ultrasound was repeated and now showed hypoechoic circumferential wall thickening (i.e., halo sign) in the bilateral axillary arteries consistent with active arteritis in those vessels (see Figure 2). He was started on 40 mg of prednisone daily to treat GCA. His symptoms and inflammatory markers improved, and he was tapered off the prednisone within the subsequent two years without incident.


