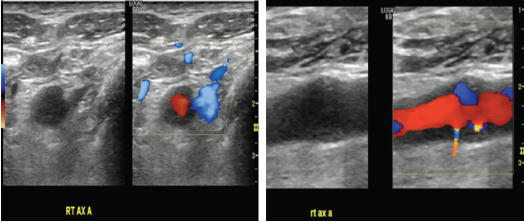
Figures 2a & 2B (from left): Vascular Ultrasound Images
Hypoechoic circumferential wall thickening of the right axillary artery is evident in transverse (A) and longitudinal (B) views.
Discussion
To our knowledge, submandibular swelling as an initial presentation of GCA has been reported only three times in the prior literature.1–3 In two of those cases, diagnosis of GCA was made on the basis of submandibular gland histopathology, as in our patient, and in the third, GCA was diagnosed on temporal artery biopsy. Clinical presentation in these reported cases varied with respect to presence of classic GCA features and inflammatory markers.
Ruiz-Masera et al. reported a case of a 75-year-old woman who presented with a painful right-sided submandibular mass; she had no systemic symptoms of GCA, and her ESR was normal.1 A resection of the submandibular gland mass showed GCA. Five months later, she developed symptoms of systemic GCA with headache, fever, fatigue, arthralgias and elevated ESR, and was treated with steroids.


