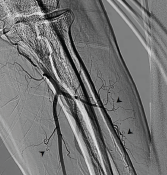
Figure 2. Invasive angiogram of left brachial artery terminating into the radial and ulnar arteries. Note the multiple corkscrew collateral vessels off the radial and ulnar arteries (arrowheads).
The patient had decreased hand pain with nifedipine and sildenafil. After several days, his right second digit began spontaneously draining serosanguinous fluid, which was cultured and grew Klebsiella oxytoca. The patient’s antibiotics were tailored to an oral regimen based on antimicrobial susceptibilities, and he was discharged. After one month, in outpatient follow-up, the patient’s digital ulcerations had improved with oral vasodilators. Despite counseling, he continued to regularly smoke blunts filled with cannabis.
Discussion
In this case, we have objective evidence of distal-extremity ischemia in the form of multiple subacute digital ulcerations and underlying acro-osteolysis on X-ray in the setting of regular cannabis exposure. This constellation of features raises the possibility of cannabis arteritis. However, cannabis arteritis is a diagnosis of exclusion.7 After thorough assessment, no evidence supported autoimmune disease or hypercoagulable state as the cause of his presentation.
A hypercoagulable state was likewise unlikely. The patient had no history of venous or arterial thrombosis, and antiphospholipid antibodies were not detected. A proximal source of emboli was not found on either transthoracic echocardiography or invasive angiogram, where vessels proximal to the elbow were largely patent on both arms. No significant proximal atherosclerosis was seen on invasive angiogram. Further, his invasive angiogram was highly consistent with cannabis arteritis given the diminished distal flow and numerous corkscrew collateral arteries.1,7
The patient did not have diabetes mellitus given his normal fasting serum glucose levels; diffuse atherosclerotic disease in the setting of diabetes mellitus as a mimic of the invasive angiogram findings was, therefore, unlikely. Despite the patient’s age of 61, older than the mean age at presentation for cannabis arteritis in the literature, cannabis arteritis was the most appropriate diagnosis in this case.
To our knowledge, cannabis arteritis has only rarely been reported in the complete absence of any concomitant tobacco use.3,4 Therefore, in our case, the lack of any history of associated tobacco exposure was befuddling until we discovered the patient was not just a daily cannabis user, but a daily blunt user. Although the tobacco filler in a cigar or cigarillo is removed and replaced with cannabis to make a blunt, the cigar or cigarillo wrapper is itself made of tobacco.8
Mass spectrometry shows that among commonly used cigar brands for making blunts, cigar wrappers have between 8% and 40% of the nicotine content of a standard cigarette.8 Our patient’s chosen vehicle of cannabis administration itself is made of tobacco. This case highlights the importance of explicitly asking cannabis users about their cannabis administration method to ascertain if tobacco and cannabis co-use is present via smoking blunts.
Further, the method may have implications in the prognosis of cannabis arteritis. Poor prognosis in cannabis arteritis is directly linked to continued cannabis consumption.4 Blunt smoking is associated with increased cannabis dependence, which may impede cannabis discontinuation in blunt users with cannabis arteritis.5,9
 Rachel E. Elam, MD, ScM, is an assistant professor of medicine and an adult rheumatologist at Medical College of Georgia at Augusta University and is in her first year of practice.
Rachel E. Elam, MD, ScM, is an assistant professor of medicine and an adult rheumatologist at Medical College of Georgia at Augusta University and is in her first year of practice.
 Vishal Arora, MD, is an interventional cardiologist and professor of medicine at Medical College of Georgia at Augusta University, practicing for 12 years. He serves as program director of the Interventional Cardiology Fellowship Program.
Vishal Arora, MD, is an interventional cardiologist and professor of medicine at Medical College of Georgia at Augusta University, practicing for 12 years. He serves as program director of the Interventional Cardiology Fellowship Program.
 Alyce M. Oliver, PhD, MD, is an adult rheumatologist, professor of medicine, Joseph P. Bailey, MD, Chair in Rheumatology, Division of Rheumatology and the director of the Internal Medicine Residency Program for the Medical College of Georgia (MCG) at Augusta University. She was formerly the MCG Rheumatology Fellowship program director.
Alyce M. Oliver, PhD, MD, is an adult rheumatologist, professor of medicine, Joseph P. Bailey, MD, Chair in Rheumatology, Division of Rheumatology and the director of the Internal Medicine Residency Program for the Medical College of Georgia (MCG) at Augusta University. She was formerly the MCG Rheumatology Fellowship program director.
References
- Olin JW, Shih A. Thromboangiitis obliterans (Buerger’s disease). Curr Opin Rheumatol. 2006 Jan;18(1):18–24.
- Adams MD, Earnhardt JT, Dewey WL, Harris LS. Vasoconstrictor actions of delta8- and delta9-tetrahydrocannabinol in the rate. J Pharmacol Exp Ther. 1976 Mar;196(3):649–656.
- Peyrot I, Garsaud A-M, Saint-Cyr I, et al. Cannabis arteritis: A new case report and a review of literature. J Eur Acad Dermatol Venereol. 2007 Mar;21(3):388–391.
- Cottencin O, Karila L, Lambert M, et al. Cannabis arteritis: Review of the literature. J Addict Med. 2010 Dec;4(4):191–196.
- Fairman BJ. Cannabis problem experiences among users of the tobacco-cannabis combination known as blunts. Drug Alcohol Depend. 2015 May 1;150:77–84.
- Delnevo CD, Bover-Manderski MT, Hrywna M. Cigar, marijuana, and blunt use among US adolescents: Are we accurately estimated the prevalence of cigar smoking among youth? Prev Med. 2011 Jun;52(6):475–476.
- Olin JW. Thromboangiitis obliterans (Buerger’s disease). N Engl J Med. 2000 Sep 21;343(12):864–869.
- Peters EN, Schauer GL, Rosenberry ZR, Pickworth WB. Does cannabis “blunt” smoking contribute to nicotine exposure?: Preliminary product testing of nicotine content in wrappers of cigars commonly used for blunt smoking. Drug Alcohol Depend. 2016 Nov 1;168:119–122.
- Timberlake DS. A comparison of drug use and dependence between blunt smokers and other cannabis users. Subst Use Misuse. 2009;44(3):401–415.