Her final discharge diagnosis was recurrent atrial re-entry tachycardia secondary to primary cardiac fibrosis from SSc. At her follow-up visit with a rheumatologist, the patient was feeling well without any symptoms of palpitations, presyncope, SOB or volume overload. She did not require any long-term anti-arrhythmic medication.
Awareness of cardiac manifestation is paramount, because cardiac involvement portends a poor prognosis in SSc.
Discussion
Clinical cardiac manifestations occur in 15–35% of scleroderma (SSc) patients, but the majority of SSc patients have subclinical cardiac involvement at post-mortem autopsy.1,2 Awareness of cardiac manifestation is paramount, because cardiac involvement portends a poor prognosis in SSc.2 Primary cardiac manifestations include fibrosis of the myocardium, pericardium and the conduction system, as well as heart failure and arrhythmia.1 Secondary cardiac manifestations occur secondary to pulmonary hypertension, interstitial lung disease or renal failure resulting in cardio-renal syndrome.1
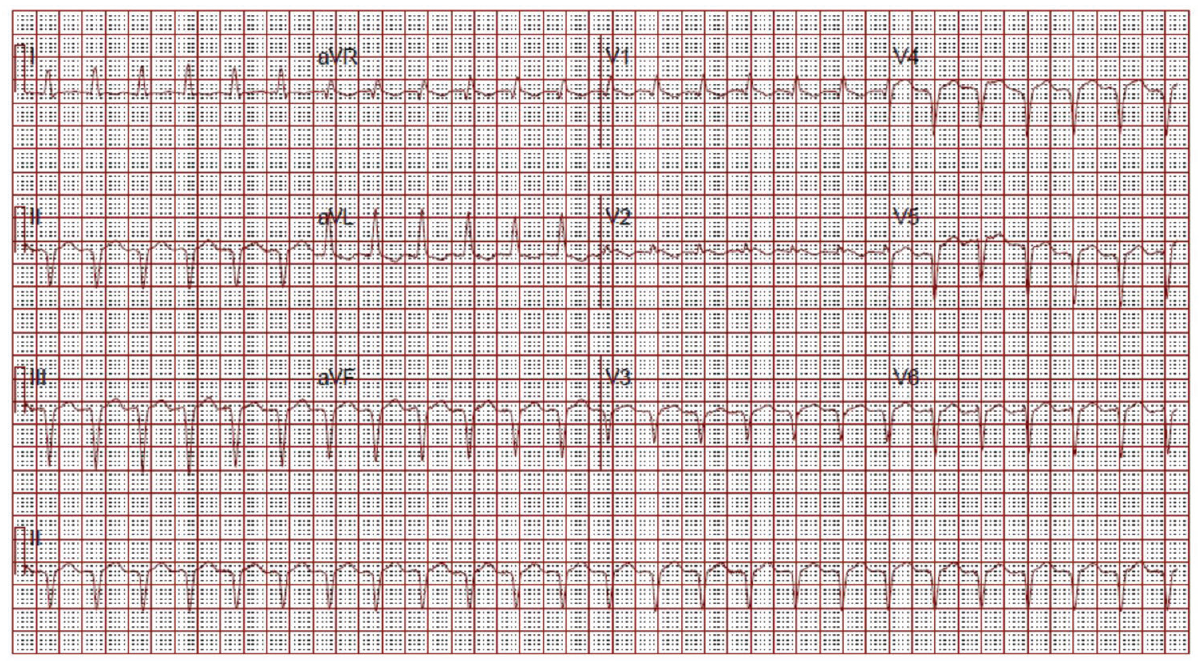
(click for larger image) Figure 2: ECG on Admission
Narrow complex tachycardia. Interpreted as sinus tachycardia.
Primary injury to an organ results in initiation of a fibrogenic response, activation of effector cells, elaboration of extracellular matrix (ECM) and dynamic deposition with insufficient resorption of ECM.3 This is no different when it comes to the heart.
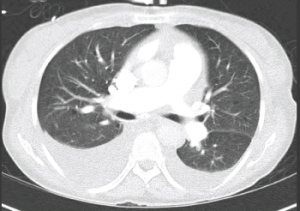
Figure 3: CT Chest
Bilateral pleural effusions. No evidence of pulmonary embolism or cardiomegaly.
As with most organs in the body, the balance of normal architecture is key in normal functioning. Cardiac cells are embedded in a collagen network made up of mostly type I (80%) and type III collagen (11%).4 This collagen network provides physical support, and also sustains transmission of evenly distributed force throughout the myocardium.4 Connexins also play a major role in propagation of electrical impulse through the heart.4 Cardiac fibroblasts are the most abundant cell type in the myocardium.3 These cells are derived from fibroblasts that are native to the myocardium, circulating in the blood or result from epithelial to mesenchymal transition (EMT).3
