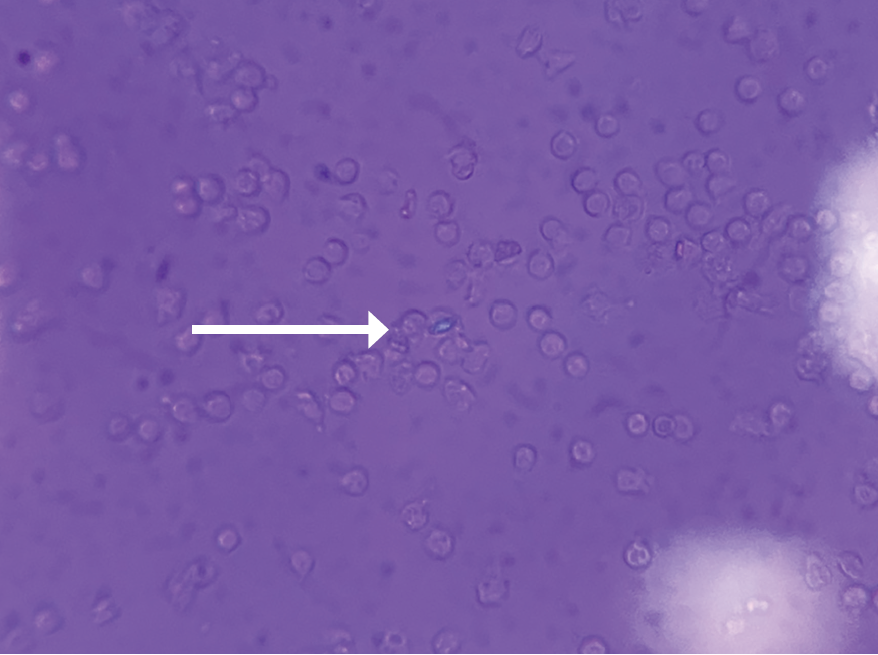
FIGURE 1 (click to enlarge): Intracellular calcium pyrophosphate crystal on polarized light microscopy.
Calcium pyrophosphate crystal deposition disease (CPPD) is an arthritis caused by the accumulation of calcium pyrophosphate crystals. Despite a prevalence of 4–7% among the adult population in Europe and the U.S., it has remained a relatively under-recognized disease owing to its many clinical presentations.1 CPPD may cause an acute mono/oligoarthritis, which may mimic gout or septic arthritis; a chronic arthritis, which may mimic a variety of chronic arthritides (e.g., rheumatoid arthritis, osteoarthritis, ankylosing spondylitis); or a systemic disease, which may mimic sepsis or meningitis. An estimated 25% of initial presentations of CPPD mimic gout or septic arthritis.1 Severity and timing of pain may truly mimic gout, but acute presentations of CPPD are typically less disabling and take longer for pain to reach peak intensity than gouty attacks.2
Although the formal diagnostic criteria have been defined, considerable practical challenges in the diagnosis of CPPD remain. Compared with urate crystals in the context of gout, calcium pyrophosphate crystals are smaller and less birefringent via light microscopy, resulting in less reliability and higher interobserver variability.3