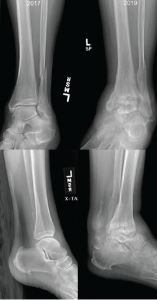
Figure 2: Comparison of X-rays
X-rays from 2017 (left) are notable for preserved joint spaces with distal fibular fracture. The 2019 X-rays (right) show diffuse, soft tissue swelling, severe erosions and talar collapse.
Pertinent lab results at the time of admission included a peripheral leukocytosis of 16.4% (109/L), with 92% neutrophils, erythrocyte sedimentation rate of 25 mm/hr and C-reactive protein of 46.4 mg/L. Arthrocentesis of the left ankle yielded 11,550 nucleated cells (differential not performed) and 25,300 red cells, with a negative gram stain and crystal analysis.
Radiographs demonstrated erosive change of the tibiotalar joints with chronic periosteal reaction and extensive soft tissue swelling, which was significantly changed from X-rays done approximately 19 months earlier (see Figure 2). Magnetic resonance imaging (MRI) showed severe erosive changes, with talar collapse, and complex tibiotalar and subtalar joint effusions, with tenosynovitis of medial flexor tendons and peroneal tendons.