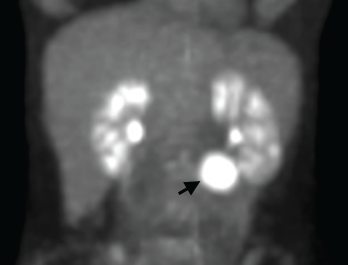
Figure 1. A positron emission tomography (PET) scan shows a 3 cm, hypermetabolic mass adjacent to the stomach.
Consulting rheumatologists often assess patients with atypical clinical presentations for the possibility of an underlying rheumatic disease. Inflammatory syndromes that are not clearly rheumatic in nature can be particularly challenging to diagnose. Here, we share the case of a young woman with a long-standing undiagnosed illness and highly elevated inflammatory markers, and describe the evaluation that led to a diagnosis of, and treatment for, unicentric Castleman disease.
Case Report
A 32-year-old woman presented to our clinic for an additional opinion. For the preceding nine years, she had experienced intermittent two- to three-month episodes of fevers, night sweats, abdominal and mid-back pain, facial rash, arthralgias and paresthesias of the extremities, without clear precipitants. Her symptoms had previously improved, in part, upon treatment with low-dose prednisone.