In addition to the GCA diagnosis, he had a past medical history of type 2 diabetes mellitus, hypertension and hyperlipidemia.
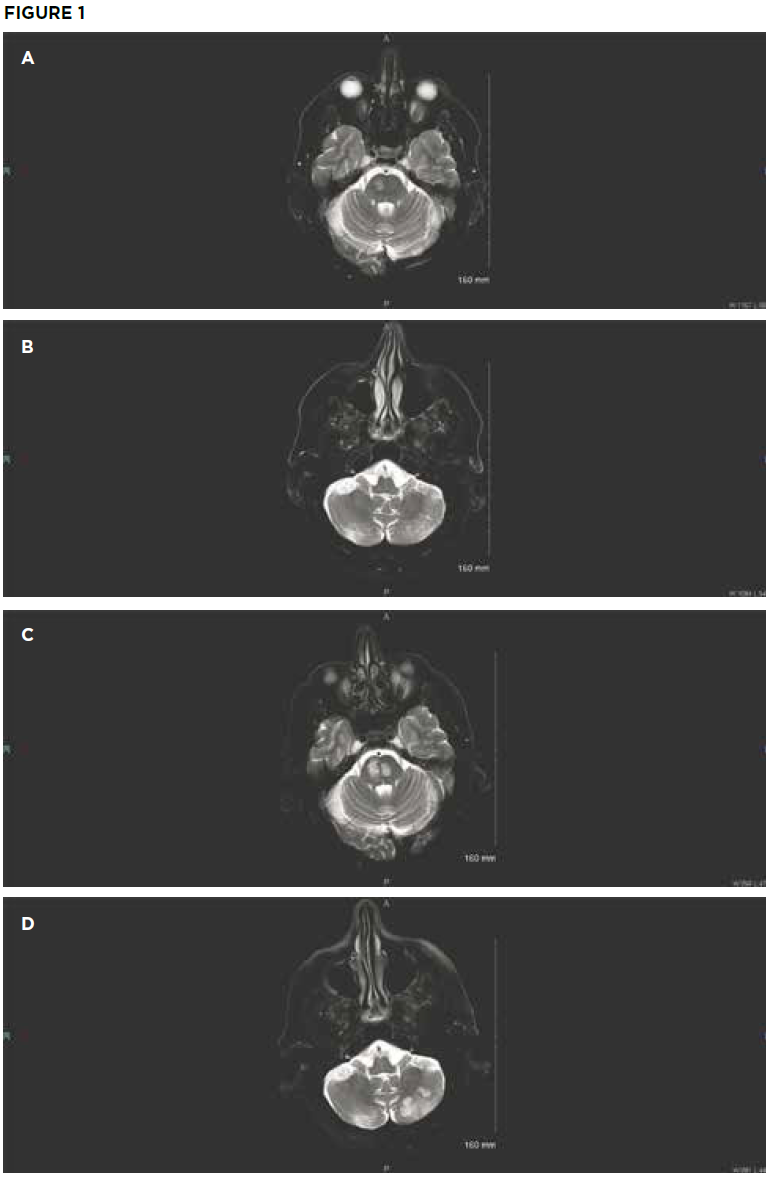
Initial brain MRI shows small areas of acute infarct in the right pons (A) and bilateral
cerebellum (B). Repeat brain MRI after sudden deterioration shows acute infarcts in the left pons with extension of infarcts in the right pons (C) and the left cerebellum (D). (Click to enlarge.)
On examination, the patient’s vital signs were within normal limits. He had severe upper and lower extremity weakness on his left side, along with left-sided facial droop and dysarthria. Laboratory testing revealed hyperglycemia of 396 mg/dL. His ESR was normal at 7 mm/hr. Throughout his emergency department stay, electrocardiograms and telemetry revealed no evidence of atrial fibrillation. Magnetic resonance imaging (MRI) showed an acute infarct in the right pons and bilateral inferior cerebellum (see Figures 1A and 1B). Magnetic resonance angiography (MRA) revealed a diminutive appearance of the vertebral arteries and the basilar artery, as well as severe bilateral siphon stenosis of the intracranial internal carotid arteries.

