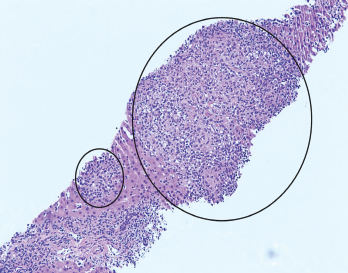
Figure 1. H&E stain at 100X showing granulomas accompanied by scattered admixed lymphocytes.
A 26-year-old woman presented to our emergency department (ED) with intermittent fevers, nausea and vomiting. She had a past medical history of well-controlled, anti-nuclear antibody positive and rheumatoid factor negative polyarticular juvenile idiopathic arthritis (pJIA) and Crohn’s disease. Her maintenance treatment consisted of monthly intravenous infliximab, 10 mg of oral methotrexate weekly and 20 mg of oral leflunomide daily.
The patient had been evaluated two weeks before at an ED in Chicago for sinus congestion and generalized malaise. She reported that a computed tomography (CT) scan of the chest showed “early pneumonia.” She was discharged home with a prescription for azithromycin for a lower respiratory tract infection and told to abstain from her immunosuppressive agents.
