and a white blood cell count of 14/hpf (RR: 0–4/hpf).
Arterial blood gas demonstrated a pH of 7.249 (RR: 7.35–7.45); pCO2 of 25.1 mmHg (RR: 35–45 mmHg); pO2; 63 mmHg (RR: 80–105 mmHg); and bicarbonate 11.0 mmol/L (RR: 24–32 mmol/L). Amylase and lipase were mildly elevated to 113 U/L (RR: 29–103 U/L) and 114 U/L (RR: 11–82 U/L), respectively. White blood cell count, blood glucose, aspartate transaminase (AST), alanine transaminase (ALT), bilirubin, alkaline phosphatase, lactate dehydrogenase (LDH), and troponin were all within normal limits.
A nasopharyngeal swab was performed and tested for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA, which was not detected.
A chest X-ray on admission showed bilateral airspace opacities (see Figure 1), and a chest computed tomography (CT) scan showed extensive diffuse groundglass opacities and cystic changes in both the upper and lower lobes of the lungs (see Figure 2).
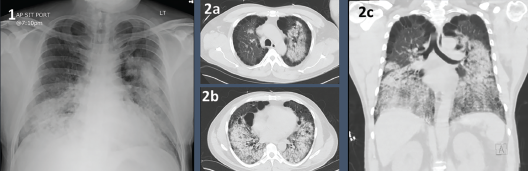
Figures 1 & 2. Figure 1: Chest X-ray with bilateral airway opacities.
Figure 2A–C: Chest CT showing extensive bilateral upper and lower lobe airway disease.


