A 65-year-old woman was referred by an orthopedist to a rheumatologist for left knee pain. Previously, in 2014, she underwent left total knee arthroplasty (TKA) for severe osteoarthritis in a different institution. Following the procedure, she experienced severe chronic anterolateral knee pain at rest, exacerbated by walking. Because she was rendered wheelchair bound and required chronic narcotic analgesia, she sought a second orthopedic opinion at our institution in 2015.
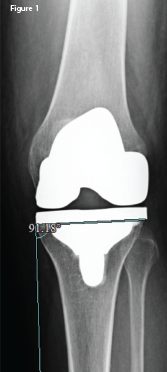
An anteroposterior X-ray of the left knee following the original arthroplasty. It shows a lateral femoral and tibial overhang of
4–5 mm and 3 mm, respectively.