MRI of the knee may define underlying pathology involving the CPN, with EPS confirming the diagnosis.2 MRI of the knee after arthroplasty may be challenging due to distortions generated by metallic artifact production, even when optimized pulse sequences are used.13
Regarding nerve damage, EPS defines abnormal function and injury location but not the underlying pathology.14
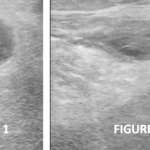
Ultrasound & the Common Peroneal Nerve at the Knee
In response to chronic compression, peripheral nerves may enlarge and/or change echotexture.15 More recently, ultrasound findings, corroborated by EPS, have been helpful in evaluating CPN neuropathy by directly visualizing the nerve and structures that may cause nerve compression.14,16-18 The most consistently reported ultrasound-measured abnormality in CPN compressive neuropathy is enlargement of the CSA of the affected CPN. In several studies, ultrasound-measured enlargement of the CSA of the CPN correlated well with abnormal EPS.14,16-18 In the largest of the studies, 87 patients with CPN neuropathy based on clinical examination and abnormal EPS were evaluated by ultrasound. Using a CPN cutoff of a CSA of 10.9 mm2, ultrasound diagnostic sensitivity was 90%, with specificity of 69%.16
However, none of the studies looked at CPN neuropathy following knee arthroplasty.
Treatment Options for Common Peroneal Neuropathy after TKA
For compressive CPN neuropathy following TKA and lasting three months or more, nonsurgical treatment (e.g., medication, splinting and physical therapy) has yielded variable results.1,19,20 Surgical decompression of the common peroneal nerve after TKA has more consistently produced successful results, although large studies are lacking.1,19,20
Is Knee Arthroplasty Component Overhang Important?
The relation of tibial and femoral component overhang to pain and outcome after TKA is a topic of interest beyond the scope of this discussion.21-23 However, in our single case, correction of the femoral component overhang alone was insufficient for a good outcome. Our patient achieved marked pain relief when both the lateral tibial and femoral component overhang and the varus deformity were corrected.
Conclusion
The clinical presentation of CPN neuropathy after TKA may present atypically, with only pain and/or decreased knee range of motion.1 This presentation without nerve palsy or paresthesias is termed CPN dysfunction and may be considered a subset of CPN neuropathy.1 Ultrasound examination of the CPN, quantitating CSA and comparing it with the unaffected nerve may be useful to evaluate for CPN compressive neuropathy in cases of TKA with suboptimal results. Confirmation with EPS is still necessary.
Regarding compressive neuropathies, ultrasound and EPS are complementary; the former assesses morphology, and the latter measures physiologic nerve function.18 Surgical decompression appears to be the most successful treatment option for CPN compressive neuropathy with either classic neuropathy or dysfunction.19,20
To the best of our knowledge, this is the first reported use of ultrasound as the initial screening modality for CPN dysfunction after TKA.
Mark H. Greenberg, MD, RMSK, RhMSUS, is board certified in internal medicine and rheumatology. He is an associate professor of medicine at the University of South Carolina School of Medicine at Palmetto Health USC Medical Group, Columbia, S.C.
Elijah Mitcham, MD, graduated from Mercer University School of Medicine, Georgia, and completed his internal medicine residency at Palmetto Health/University of South Carolina.
Prem Patel is a medical student at the University of South Carolina School of Medicine, Columbia. He graduated from the University of South Carolina with a BS in biomedical engineering.
James W. Fant Jr., MD, is board certified in internal medicine and rheumatology. He is an associate professor of medicine at the University of South Carolina School of Medicine and director of the Rheumatology Division at Palmetto Health USC Medical Group, Columbia, S.C.
Frank R. Voss, MD, is an associate professor of orthopedic surgery, director of medical education for orthopedic surgery and the department’s vice chair at the University of South Carolina School of Medicine. He is board certified in orthopedic surgery.
References
- Zywiel MG, Mont MA, McGrath MS, et al. Peroneal nerve dysfunction after total knee arthroplasty: Characterization and treatment. J Arthroplasty. 2011 Apr;26(3):379–385.
- Baima J, Krivickas L. Evaluation and treatment of peroneal neuropathy. Curr Rev Musculoskelet Med. 2008 Jun;1(2):147–153.
- Clark NE, Bobo LS, Ho CA. Knee dislocation with common peroneal nerve rupture. International Journal of Athletic Therapy and Training. 2013;18(5):29–31.
- Coraci D, Tsukamoto H, Granata G, et al. Fibular nerve damage in knee dislocation: Spectrum of ultrasound patterns. Muscle Nerve. 2015 Jun;51(6):859–863.
- Dan C, Ispas AT, Vasilescu M, et al. Sport related injuries of the nerves in the knee region. Medicina Sportiva. 2014;