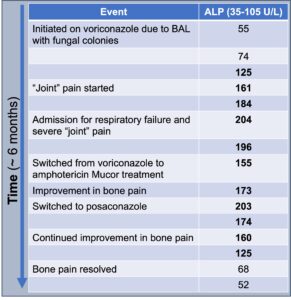
Figure 4
ALP trends over time
Clinically, symptoms of VIP include diffuse, often severe, and constant bone pain that worsens with palpation. In severe cases of periostitis, palpable bony overgrowth and nodules can occur. Joint swelling has been reported, as have non-specific symptoms of myalgias and weakness. The pain tends to be minimally responsive or unresponsive to steroids, colchicine, and opiates. Although any bone can be affected, the ribs, proximal long bones, shoulders and hands are most commonly involved. Excess fluoride can also deposit on dental enamel, resulting in dental fluorosis characterized by white streaks or specks.3,4
