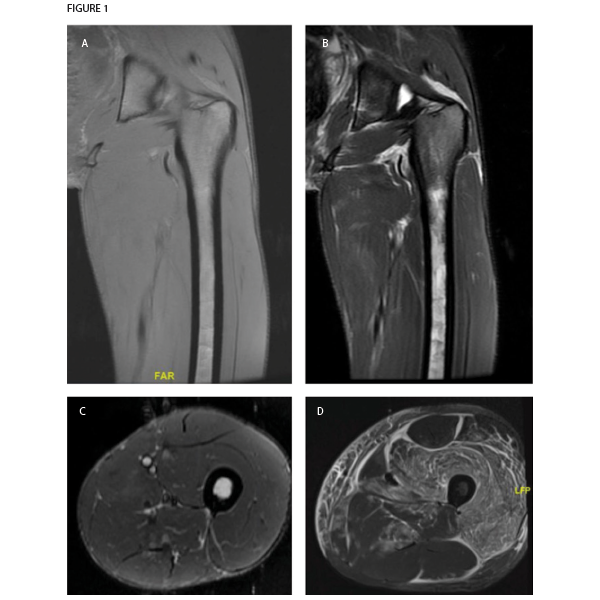
Figure 1. Magnetic resonance imaging of patient’s left thigh. Coronal sections of (A) T1-weighted and (B) T2-weighted sequences both demonstrate extremely thin layer of subcutaneous fat, also seen in the (C) axial section section of STIR sequence imaging. The muscle parenchyma does not have any regions of high T2 signal intensity to suggest muscle edema, as is seen in an axial STIR image from a representative patient with dermatomyositis (image courtesy of Simon Helfgott, MD) (D). The patient’s bone marrow has low T1 and high T2 and STIR signals in the diaphysis of the femur, consistent with serous atrophy. Normal bone marrow has high T1 signal and low T2 and STIR signals.
Our list of differential diagnoses also included occult malignancy, especially in light of the pancytopenia. Lactate dehydrogenase was 182 units/L. The patient refused a bone marrow biopsy. Recent upper and lower endoscopy results were normal. Computed tomography (CT) of the chest, abdomen and pelvis did not suggest malignancy, but was notable for diffuse abnormal appearance of the muscles of the chest, potentially consistent with myositis or myopathy.
An MRI of the thigh was obtained to further characterize the muscle abnormality initially seen in the CT scan. Notably, the muscle parenchyma itself was completely normal, with no signs of edema or fatty replacement. Instead, the MRI revealed a marked decrease in subcutaneous fat. Also, T2 signal hyperintensity was present in the bone marrow of the femur, consistent with serous atrophy. No fractures were seen.


