SAN DIEGO—Rheumatologists may encounter patients with systemic disease who present with various forms of alopecia that seem sudden or unusual. Hair loss can be caused by autoimmune inflammation in some cases, but there are many other potential causes that a rheumatologist must explore to treat the condition effectively.
Rheumatologists often may see a patient presenting with a complaint of hair loss, especially those with autoimmune diseases like systemic lupus erythematosus (SLE) or rheumatoid arthritis (RA), said Maria K. Hordinsky, MD, chair of the department of dermatology at the University of Minnesota in Minneapolis during her presentation at the 2013 ACR/ARHP Annual Meeting. “Even though you have done a great job of treating their connective tissue disease,” alopecia can still occur. [Editor’s Note: This session was recorded and is available via ACR SessionSelect at www.rheumatology.org.]
Hair Sheds Daily
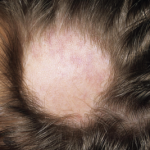
Looking at a cross-section image of a normal scalp, about 90% of the hair follicles look the same, Dr. Hordinsky said. However, hair shedding and even pattern baldness are common among almost all adults. “Every day, we shed hair fibers. There is always recycling going on,” she said. Hair production goes through three cycles: anagen (actively growing), catagen (involution of growth), and telogen (resting). Telogen effluvium is the general term for pattern hair loss. “When patients come to you complaining that their hair is coming out at the roots, what they are losing are the telogen fibers,” she said. Stem cells are located in the bulge region near the base of the hair follicle, she noted.
Alopecia has a psychological impact for many patients, and they may try to hide their hair loss with caps, scarves, or hairpieces. It’s important for rheumatologists to not assume telogen effluvium is simply female pattern baldness but to examine the scalp closely and consider many possible causes, Dr. Hordinsky said. Ascertain if the patient’s family has a history of baldness, and also check for nail abnormalities, menstrual irregularities, or pregnancy, as well as asking about excess body hair, which the patient may have waxed or shaved, she suggested.
Looking closely at the scalp for symptoms like burning, pruritus, pain, redness, scaling, folliculitis, or scarring may provide more clues to the cause of the hair loss. Look at the pattern of hair loss as well as whether or not there is new hair growth visible. A “pull test” is standard. If six or more hairs from any site on the scalp fall out with gentle pulling, this is a sign of diffuse alopecia areata (AA), an autoimmune disease, she said. Standardized scales help categorize the level of alopecia; female pattern baldness is measured on the Ludwig scale, and male pattern baldness is measured on the Hamilton-Norwood scale.
Hair shedding is a common symptom of hypothyroidism, so ordering thyroid-stimulating hormone screening may be useful, Dr. Hordinsky said. Other tests that may offer clues are a complete blood count, ferritin measurement, and antinuclear antibody, as well as measuring for abnormal levels of vitamins D and E, thiamine, zinc, and total protein, she noted.
There are a number of inflammatory alopecias, Dr. Hordinsky said. Cicatricial alopecia presents with scalp scarring and hair loss. The inflammatory processes in cicatricial alopecia may be lymphocytic or neutrophilic. Lichen planopilaris is a common lymphocytic alopecia that presents with a red, itchy, burning scalp. The inflammatory process presents at the bulge region where the stem cells are located. Treatments include topical corticosteroids, intralesional corticosteroids, and topical nonsteroidal antiinflammatory drugs, as well as oral medications such as hydroxychloroquine, low-dose antibiotics, and corticosteroids.
Standard treatments for noninflammatory alopecia include minoxidil, which may be oral or topical. Hair-replacement surgery is another option, as are newer laser combs and low-level laser therapy, the latter of which has shown promise, Dr. Hordinsky said. Cosmetic interventions include shampoos or other hair-care products that help hair appear thicker.
Examine for Patterns
It’s important to examine the pattern of the hair loss on the scalp, Dr. Hordinsky said. Rheumatologists may see telogen effluvium in patients with chronic cutaneous lupus and especially in those with discoid lupus, whose hair loss often is seen at the crown of the head, Dr. Hordinsky said. In SLE, hair loss may be all over the scalp. In a female with perifollicular inflammation, scarring may progress from front to back on the scalp, she said. Frontal fibrosing alopecia (FFA) is a condition presenting with scarring and hair loss at the forehead that occurs most commonly in postmenopausal females. Newer therapies for FFA include anti-androgen therapy and pioglitazone (Actos), which is widely used for type II diabetes, she said.
Alopecia areata, an autoimmune disease presenting with anagen effluvium, may be connected to RA based on data from genome-wide studies, Dr. Hordinsky said. Currently, there is no U.S. Food and Drug Administration–approved treatment for AA. In patchy AA or ophiasis AA, marked by hair loss at the circumference of the scalp, potential treatments include corticosteroids, minoxidil, anthralin (Psoriatec), and steroid shampoos. Treatments may include corticosteroids such as intralesional kenalog at 4 ccs injected at a 45-degree angle at the site of the hair loss every six weeks. “What is much more challenging is when alopecia areata is much more extensive and occurs all over the body,” she noted. In conditions like alopecia areata totalis or universalis, corticosteroids may also be used as well as immunotherapies like methotrexate, cyclosporine, sulfasalazine, or biologic drugs. In such cases, “we will do a scalp biopsy in our clinic, but the hair follicles are so small that they are barely visible,” Dr. Hordinsky said.
To identify the genetic causes of AA, a related registry was started in 2000; 3,513 patients have completed the registry so far, she added. Eight genes have been identified as contributing to AA, including cytotoxic T lymphocyte–associated protein 4, interleukin (IL) 2, and human leukocyte antigen, which are also associated with RA. However, newer research points to ULBP3 as major culprit in AA, and higher levels of the gene were found expressed in hair follicles in AA. “People have always described alopecia areata as a cluster of bees swarming around the base of the hair follicle,” Dr. Hordinsky said. “Now, we believe that ULBP3 is the honey that attracts the lymphocytes, or the bees.” Emerging therapies for AA may target inflammatory cytokines like IL-15 or janus kinase, but more studies are needed.
When counseling patients presenting with hair loss, addressing hair-care habits is essential, Dr. Hordinsky concluded. Styling routines like using hair dryers on high heat settings, flat ironing or using curling irons, or even vigorous brushing and tight “ponytail” hairstyles can damage or pull out hair, she noted.
“The hair follicle is a highly complex structure,” Dr. Hordinsky stressed. “Many things can go wrong, so use the tools available.”
Susan Bernstein is a writer based in Atlanta.