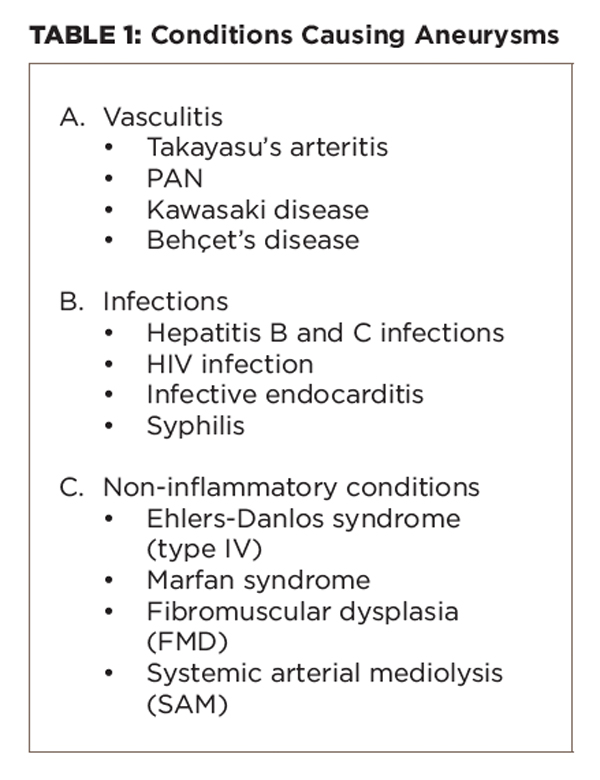
Important differential diagnoses that cause aneurysms are given in Table 1.
(click for larger image)
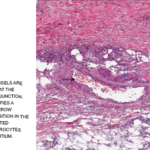
Aneurysms occur in the other forms of vasculitides, as well. In Takayasu’s aortoarteritis (large vessel vasculitis), aneurysms are well described in the aorta and its major branches in the proximal portions of these vessels on angiography, and rarely, there are aneurysms of the visceral arteries.4 It usually presents with limb claudication, CNS ischemic symptoms, absent or unequal pulsations and hypertension. Pulmonary artery aneurysms presenting in the midpart of the pulmonary artery, presenting with hemoptysis is typical of Behçet’s disease (variable vessel vasculitis) and is associated with the predominant mucocutaneous and ocular features.1 Kawasaki disease (medium vessel vasculitis) is characterized by coronary artery aneurysms in children.1