On MRI, she was found to have cortical restriction with increased T2 signaling of the left temporal lobe, left insula and left frontal lobe.
Doctors were now concerned about autoimmune encephalitis or infection, and she was transferred because the community hospital where she was had no infectious disease or rheumatology department. At the new center, the girl was agitated, was asking that music be turned off when none was playing, and she didn’t recognize her parents.
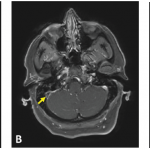
Another MRI found progressive disease that was bilateral, but worse on the left, with leptomeningeal enhancement in the wake of seizures.
Possible Autoimmune Encephalitis
Criteria for possible autoimmune encephalitis (AE) are rapid progression of working memory deficits in less than three months, altered mental status or psychiatric symptoms, one or more of new focal central nervous system findings, seizures unexplained by a previous disorder, a white blood cell count of more than 5 cells per cubic millimeter, MRI features suggesting encephalitis, and “reasonable exclusion of alternative causes,” which Dr. Wells called, “the tricky part.”1
Meeting these criteria is “not a diagnosis in and of itself,” but is only a guide signaling the clinician to “think about autoimmune encephalitis,” Dr. Van Mater said.
For definite autoimmune encephalitis, the history, exam and labs all need to be consistent with AE, with no other clear diagnosis, and a positive anti-neuronal antibody; a patient has probable AE when his or her history, exam and labs are all consistent with AE, with no other clear diagnosis, but is negative for an anti-neuronal antibody.
Anti-NMDA-Receptor Encephalitis
A diagnosis of anti-N-methyl D-aspartate (NMDA) receptor encephalitis requires meeting these three criteria: 1) Onset in less than three months of four of these six symptoms: abnormal behavior or cognitive dysfunction, speech dysfunction, seizures, a movement disorder or dyskinesia, a decreased level of consciousness and autonomic dysfunction, or central hypoventilation; 2) an abnormal electroencephalogram and/or abnormal cerebrospinal fluid pleocytosis or oligoclonal bands; and 3) reasonable exclusion of other disorders.
Diagnosing autoimmune brain disease can be challenging because patients’ phenotypes overlap, Dr. Van Mater said.2
“There’s such overlap in their ultimate diagnosis based on phenotype alone that you have to do a pretty broad evaluation to make the diagnosis,” she said.
After a positive anti-nuclear antibody test and an extensive infectious disease workup that was negative, clinicians continued to ponder the diagnosis, with at least some factors both supporting and running counter to diagnoses of primary central nervous system (CNS) vasculitis, autoimmune encephalitis, systemic rheumatic disease, demyelinating disease, para-infectious and active bacterial infection.