In another study among multiple myeloma patients treated with zoledronic acid or pamidronate, the authors found 10 known SNPs involved in bone turnover associated with MRONJ.30 The genes included COL1A1, CYP2C8, MMP2, OPG, OPN, RANK and TNF.31
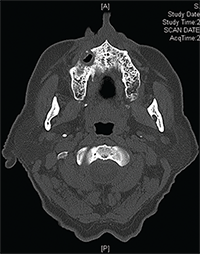
Figures 3A & B: Maxilla involved by osteonecrosis: (top) necrotic bone of right maxilla; and (bottom) bone defect of right maxilla with maxillary sinus involvement.
Another genome-wide association study showed that individuals with an SNP in the RBMS3 gene (associated with collagen formation and bone density) were approximately six times more likely to develop MRONJ.32


