The Case
A 25-year-old, previously healthy, white male presented to our hospital with fever, cough, nausea and vomiting of several weeks duration. He reported a 35 lb. weight loss over the previous year and had recently developed painful oral ulcers. Roughly three weeks prior to admission, he had seen a gastroenterologist for these complaints and was found to have anti-tissue transglutaminase IgA antibodies (anti-TGA IgA) consistent with a diagnosis of celiac disease.
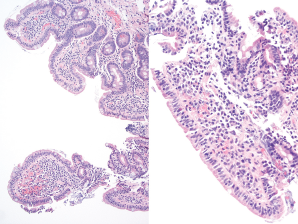
Figure 1. Duodenum biopsy showing partial villous atrophy with borderline increase in intraepithelial lymphoctyes.
An esophagogastroduodenoscopy was performed on an outpatient basis, with findings that could be compatible with malabsorption, possibly due to celiac sprue (see Figure 1). He refrained from eating gluten and his symptoms improved.