Finally, the researchers determined rates of adverse events potentially attributable to TMP-SMX during person-time exposed and unexposed to TMP-SMX.
Results
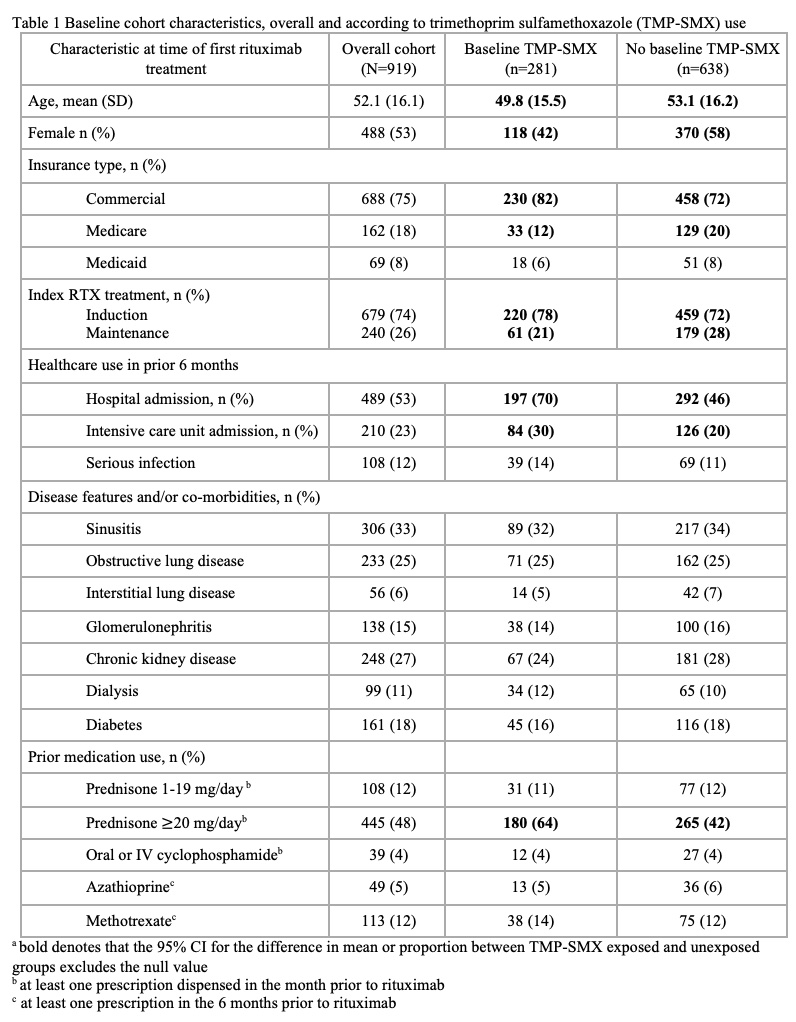
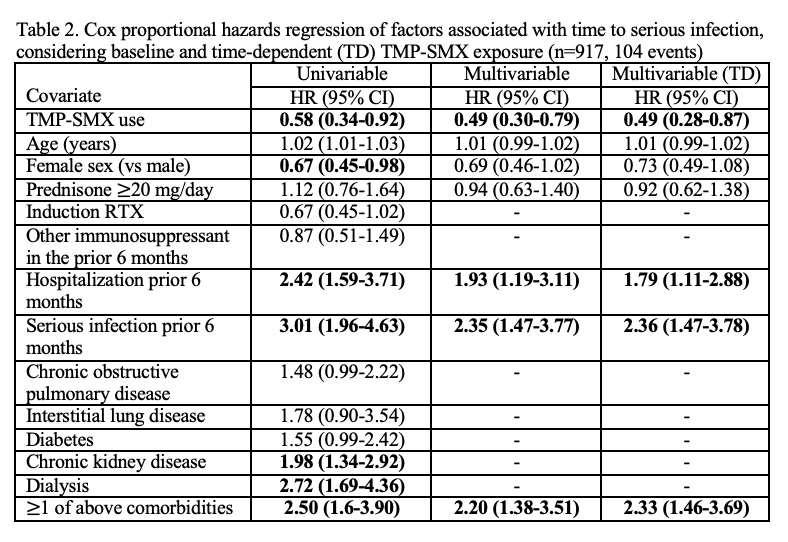
The cohort included 919 individuals with GPA—mean age 52 years (SD 16)—who were treated with rituximab. Fifty-three percent were women. TMP-SMX was dispensed to 281 (31%) at the time of the index rituximab (and to 40% on prednisone ≥20 mg/day). Over a median (IQR) follow-up of 496 (138,979) days, the rates of serious infection, outpatient infection and PJP per 100-person years were 6.1 (95% confidence interval, CI 5-7), 28.7 (95% CI 26–32), and 0.7 (0.4–1.2), respectively. Serious infections were primarily pulmonary (36%) or general sepsis (45%). In multivariable analyses, TMP-SMX was negatively associated with serious infections, considering baseline (adjusted HR 0.5; 95% CI 0.3–0.8) and time-varying TMP-SMX exposure (aHR 0.5; 95% CI 0.3–0.9). Prophylaxis was also negatively associated with outpatient infections (aHR 0.7; 95% CI 0.5–0.9). Thirteen pneumocystis jirovecii pneumonia infections occurred, all in subjects who were not exposed to TMP-SMX. TMP-SMX was not associated with reduced HZ (aHR; 1.6, 95% CI 0.6–3.2). Rates for adverse events potentially attributable to TMP-SMX per 100 person-years were 29.6 (95% CI, 22–39) during periods of TMP-SMX exposure and 13.4 (95% CI, 11–16) during periods without TMP-SMX exposure.
Conclusion
TMP-SMX prophylaxis was associated with subsequent reduced serious and overall infections in patients with GPA treated with rituximab. Further study is needed to determine how to balance potential benefits and harms from prophylaxis in individual patients and determine optimal prophylaxis duration.
Disclosures
A. Mendel: None; H. Behlouli: None; E. Vinet: None; J. Curtis: AbbVie, 2, 5, Amgen, 2, 5, Bristol-Myers Squibb, 2, 5, CorEvitas, 2, 5, Eli Lilly and Company, 2, 5, Janssen, 2, 5, Myriad, 2, 5, Novartis, 2, 5, Pfizer, 2, 5, Sanofi, 2, 5, UCB, 2, 5; S. Bernatsky: None.
Mendel A, Behlouli H, Vinet E, Curtis J, Bernatsky S. Effect of trimethoprim sulfamethoxazole prophylaxis on infections during treatment of granulomatosis with polyangiitis with rituximab: A population-based study [abstract]. Arthritis Rheumatol. 2023;75(suppl 9).



