(click for larger image)
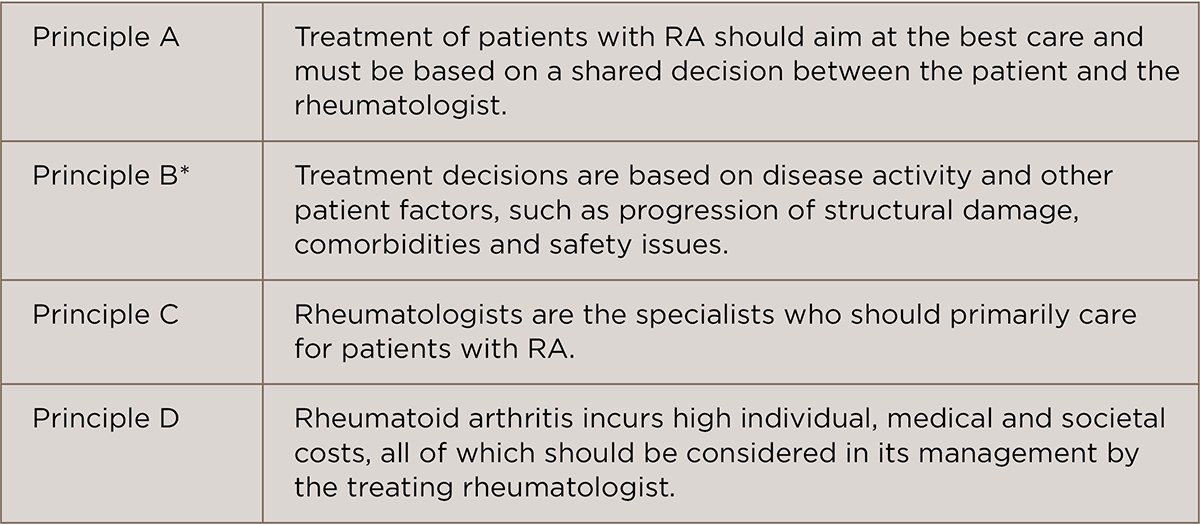
TABLE 1: EULAR 2016 RA Guidelines: Overarching Principles4
*New principle added
Commenting on the guidelines, Vivian P. Bykerk, MD, director of the Inflammatory Arthritis Center, Hospital for Special Surgery, and an associate professor of the Weill Cornell Medical College, New York, highlighted that a significant conceptual change in the guideline is that the goals for therapy will need to be considered in light of any patients with comorbid conditions. “That is not to say that the goal of sustained disease control should not be aimed for, but that it is reasonable not to escalate therapies to try and achieve stringent disease control if it would not be safe to do so if a comorbid condition places the patient at greater risk for an adverse event,” she says.
Specific Treatment Recommendations
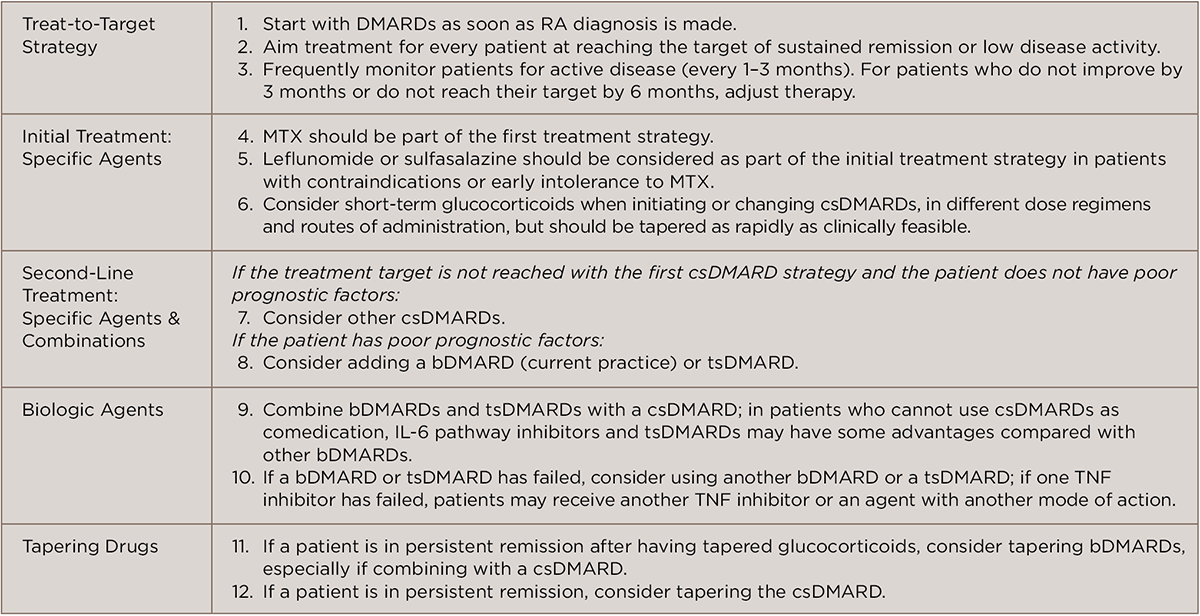
Similar to the previous guidelines, the 2016 recommendations are based on an overall treat-to-target strategy that begins with initiating effective disease-modifying anti-rheumatic drug (DMARD) therapy immediately following a diagnosis of RA, setting a treatment target goal, and assessing disease activity while trying to reach the target goal (see recommendations 1–3 in Table 2).
(click for larger image)
TABLE 2: EULAR 2016 RA Guidelines: Treatment Recommendations4
Glossary: DMARDs, disease-modifying anti-rheumatic drugs; RA, rheumatoid arthritis; MTX, methotrexate; csDMARDs, conventional synthetic DMARDs; bDMARD, biologic DMARD; tsDMARD, targeted synthetic DMARD; TNF inhibitor, tumor necrosis factor inhibitor
According to Dr. Bykerk, a key conceptual change in this guideline is to extend the goal of therapy to include the word sustained. “Thus, not only do we want a patient to achieve a target goal of remission, or if that is not possible then low disease activity, but we expect the patient to be regularly monitored and medication adjustments performed to maintain that target goal,” she says.
Other significant changes in this guideline from previous guidelines are new recommendations on the types of agents to use and when. One changed recommendation the lead author of the guidelines, Josef Smolen, MD, professor, Division of Rheumatology, Department of Medicine 3, Medical University of Vienna, Austria, highlights is the recommendation that initial therapy to treat treatment-naive patients can be with methotrexate (MTX) plus short-term glucocorticoids.