click for large version
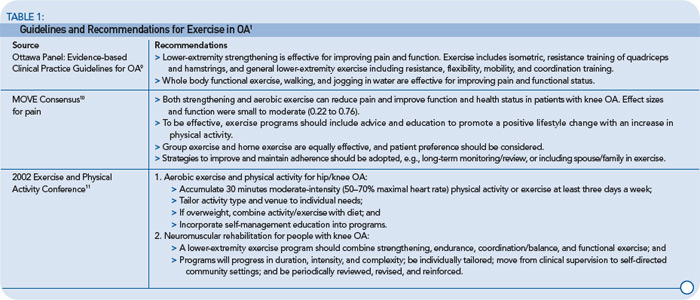
TABLE 1. Guidelines and Recommendations for Exercise in OA1
Promote Exercise at the Office Visit
In general, people who receive advice from their physician to exercise are more likely to exercise than people who do not. People with arthritis who exercise often begin because a physician suggested it and provided information. In a study of rheumatologists and patients with rheumatoid arthritis, only 58% of the physicians discussed exercise with their patients, and most physicians reported that they did not have the time or feel comfortable recommending exercise.5 To follow current management guidelines for knee OA, exercise should be discussed at every office visit. It is up to the physician to start the discussion.

