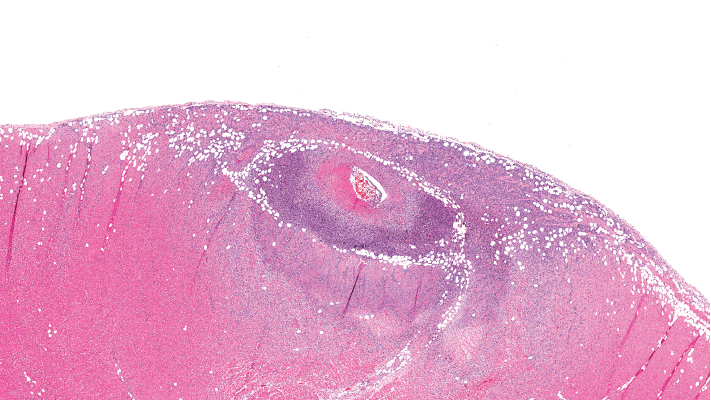
This image depicts severe arteritis of the coronary artery with inflammation and thrombosis, with extension into the myocardium.
A proposed model to predict the risk of giant cell arteritis (GCA) prior to a temporal artery biopsy could help triage patients and guide decision making about the need for biopsy or monitoring (see Figure 1).
There’s no specific biomarker for GCA, and GCA can be a “diagnostic conundrum, especially when it presents in an occult or atypical fashion,” according to the researchers who published the development and validation data on their multivariable prediction model in a recent issue of Clinical Ophthalmology.1

