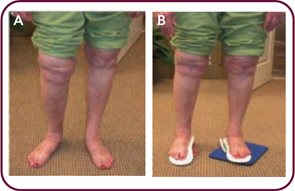
Figure 1: Alignment problems associated with different leg lengths. A) Significantly longer right leg as a result of bilateral hip and knee replacements. B) Improvement in alignment with leg length and pronation correction.
Role of Malalignment in OA Pathogenesis
I am not a research scientist, but I have the utmost respect for those who are. I’m a clinician who, for the last forty years, has been treating patients, reading the literature, and simply observing how people function every day. My perspective is different because I have subspecialized in a number of seemingly unrelated areas of medicine. In each instance, the thing I was interested in least—biomechanics—was the common thread that haunted me. Yet nowhere have I found the importance of controlling pathomechanics more applicable than in rheumatology.

