click for large version
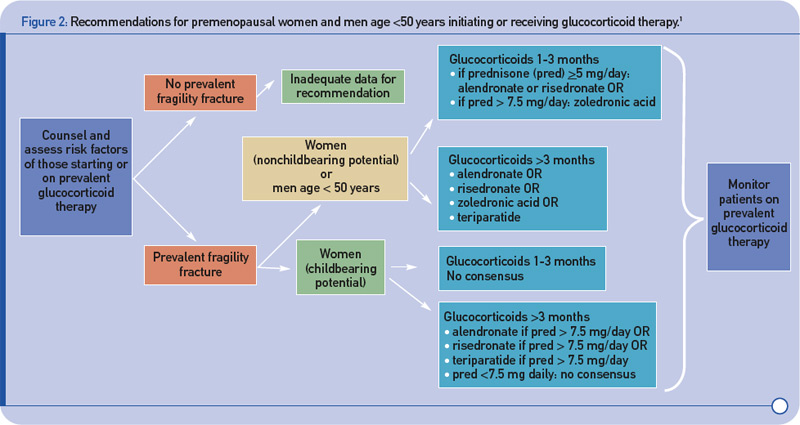
Figure 2: Recommendations for premenopausal women and men age <50 years initiating or receiving glucocorticoid therapy.1
Women with childbearing potential and a history of fragility fracture who take 7.5 mg or more of prednisone per day can also be treated with alendronate, risedronate, or teriparatide. No recommendations are given for premenopausal women or men under age 50 with no history of fracture because the evidence is currently inadequate. “This is a population where a case-by-case determination needs to be made. Depending on their risk factors, bone mineral density measurements, and pregnancy plans, we may want to follow their bone mineral density more closely to see whether these studies are showing a decline if they are not on therapy,” Dr. Grossman says.

