Gout flares will self-resolve, even in the absence of treatment, Dr. Poulson explains. Many of the mechanisms involved in initiating the inflammatory cascade in the gout flare also trigger pathways to turn it off, ensuring that inflammation can only persist for a finite period.
“For instance, NLRP3 inflammasome activation results in self-cleavage of the enzyme caspase 1. This activates caspase 1, allowing it to then activate IL-1β, a key step in initiating the inflammatory cascade in the gout flare. However, self-cleavage also targets caspase 1 for destruction, ensuring that caspase 1 activity is self-limiting,” Dr. Poulson says.
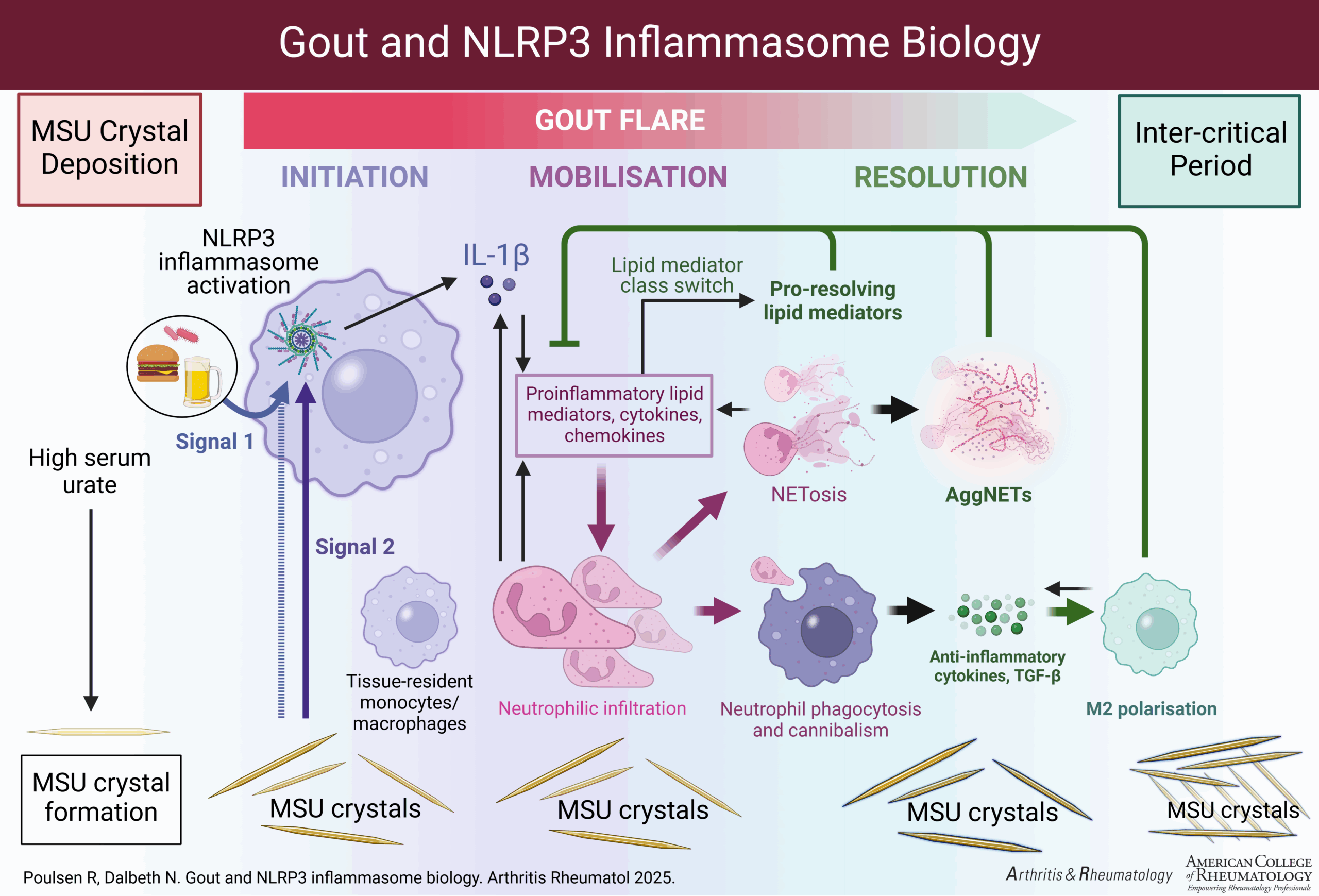
Click to enlarge.
Neutrophil activation and the resultant increased production of inflammatory cytokines plays “a central role in amplifying the inflammatory response in the gout flare and is associated with the increased intensity of symptoms during initial gout flare development. However, neutrophils are also critical for flare resolution,” Dr. Poulson explains. Aggregated neutrophil elastase traps (NETs) are “released by neutrophils sequester chemokines and inflammatory cytokines. As NETs accumulate, they also form a coating on MSU crystals, reducing the inflammasome-activating ability of the crystals. Neutrophils undergoing apoptosis at the end of their life cycle are a major source of anti-inflammatory mediators, such as TGF-β [transforming growth factor beta], which is key for driving a switch in macrophage polarization from M1 to M2.”
Case Study
In the clinical case, a 60-year-old man presented with a six-hour history of pain and swelling in his right, first metatarsophalangeal (MTP) joint. He described a throbbing sensation in his big toe joint that woke him overnight. Over one hour, he developed intense pain—described as the worst he had ever experienced, with 9/10 in severity—redness, heat and swelling in the joint. The patient could not move the joint, put weight on his foot or wear a shoe.
