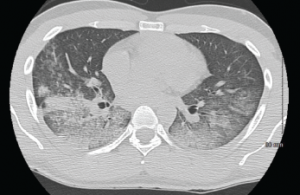
A CT scan of the chest showing multifocal ground-glass opacities, representative of hemorrhage, with numerous nodular interstitial opacities primarily within a peribronchovascular distribution.
A 22-year-old Indian male presented to the emergency department with hemoptysis. A month prior, he had presented to an urgent care center complaining of cough with occasional episodes of blood-tinged sputum in the morning. He was diagnosed with community-acquired pneumonia based on a chest X-ray without laboratory testing and was prescribed levofloxacin.
A few days later, he called his primary care physician for bilateral ankle pain and was told that this could be due to fluoroquinolone-induced tendinitis. The ankle pain, as well as his cough, varied in intensity before he presented to the hospital, and during this interval he also noted bilateral knee, wrist and right elbow pain. He also noted that his eyes had been “bloodshot” recently, but denied visual changes or eye pain.


