(click for larger image)
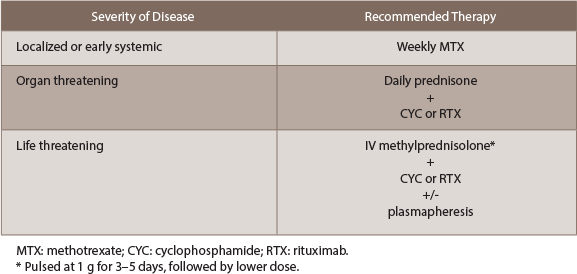
Table 1: Summary of Induction Therapy
For disease that is organ threatening, daily prednisone with the addition of either cyclophosphamide (CYC) or rituximab (RTX) is recommended. This recommendation is based on the RAVE trial, which found RTX to be noninferior to CYC. CYC can be given as either a monthly IV pulse or a daily dose, the latter offering less risk for relapse at the expense of side effects.8 With CYC, the absolute neutrophil count should be kept >1000/μL. Rituximab can be given as a weekly dose of 375 mg/m2 over four weeks or a 1,000 mg biweekly dose over two weeks. Before starting rituximab, it is imperative to test patients for hepatitis B and tuberculosis.
Patients with life-threatening disease benefit from the addition of plasmapheresis to dual corticosteroid and CYC/rituximab therapy (see MEPEX trial9). Intravenous methylprednisolone should be started immediately, at a pulse dose of 1 gram for three to five days, followed by a lower dose. If a patient is receiving both rituximab and plasmapheresis, it’s important to perform plasmapheresis first, because a portion of rituximab will be removed. The major indications for plasmapheresis are: 1) advanced kidney disease (requiring hemodialysis, creatinine >4 mg/dL or rapidly declining function); 2) positive anti-GBM antibodies; and 3) pulmonary hemorrhage.8


