Frequent complications of MD include AIP, retroperitoneal fibrosis and TIN with extraglandular involvement. Therefore, systemic examination and a fluorodeoxyglucose-positron emission tomography (FDG-PET) scan should be performed because multiple organ involvement might be present at initial diagnosis (see Fig. 1, and Fig. 2).38
First-line treatment is steroids with rapid disease response, but frequent flares can occur following discontinuation of glucocorticoid treatment.
Disease Pathophysiology
The presence of IgG4-positive plasma cells in the affected tissue and the fact that B cell depletion with rituximab (RTX) is effective in treatment suggest the importance of B-lymphocytes in the pathogenesis of IgG4-RD.39,40 Plasmablasts defined by cell surface expression of CD19, CD27 and CD38 (but negative for CD20) are elevated in the peripheral blood of patients with IgG4-RD correlating with disease activity. Because these plasmablasts demonstrate oligoclonal expansion and express IgG4, a specific antigen-driven immune response might be present in IgG4-RD.41,42
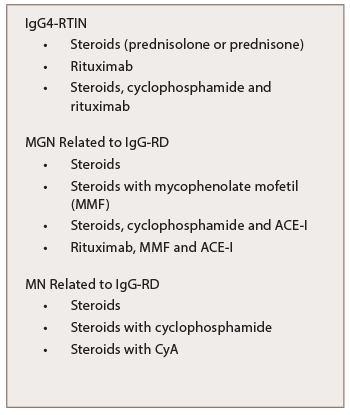
Table 7: Treatment of IgG-RKD
A Type 2 helper T cell (Th2)-driven immunological mechanism has been suggested in the pathogenesis of IgG4-RD as well.43 A clonally-expanded population of CD4+ cytotoxic T lymphocytes in the peripheral blood and fibrotic lesions of IgG4-RD patients suggest these cells are important in the disease pathogenesis by activating B cells.44 The Th2 cytokine IL-13 and the T-regulatory-associated cytokine transforming growth factor beta (TGF-β) are thought to activate fibroblasts and cause fibrosis, while the cytokines IL-4 and IL-10 might promote class-switching of IgG antibodies to IgG4 and differentiation of B cells into plasma cells. Polarized T cells possibly drive the storiform fibrosis and obliterative phlebitis observed in IgG4-RD. A separate T follicular helper cell response might generate the IgG4 phenotype.45