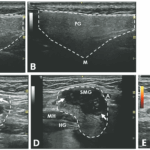
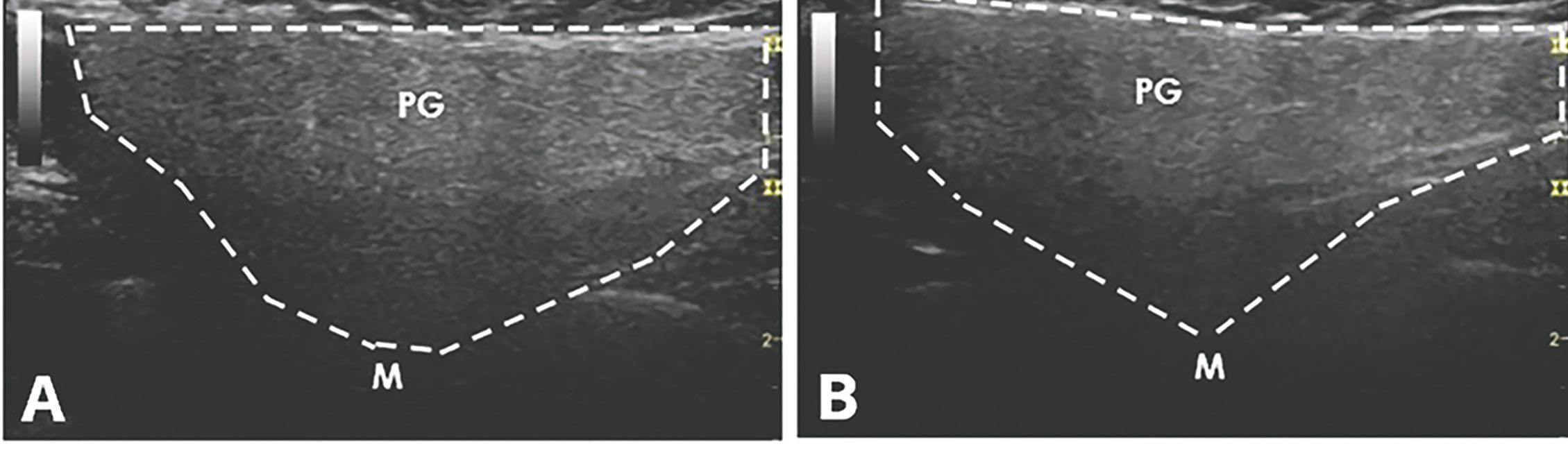
An ultrasound revealed hypoechoic nodules replacing large segments of both submandibular glands, with distortion of gland architecture, creating irregular gland surfaces and increased Doppler signal bilaterally. The parotid glands appeared normal (see Figures 1A–E).
FIGURES 1A & B: Normal longitudinal left (A) and right (B) parotid glands. (Click to enlarge.)
Laboratory testing was significant for a positive anti-nuclear antibody test at 1:160 (speckled pattern), and elevated anti-Ro/SSA antibody at 4.2 (reference range [RR]: <1.0 is negative), anti-La/SSB antibody, rheumatoid factor, thyroid-stimulating hormone, creatinine kinase and serum IgG4 level were all within normal limits. Her C-reactive protein (CRP) was normal, but her erythrocyte sedimentation rate (ESR) was elevated at 47 mm/hr (RR: 0–15 mm/hr).
A chest X-ray revealed no hilar lymphadenopathy.
Biopsy of the right submandibular gland displayed florid intralobular storiform fibrosis, and chronic lymphoplasmacytic infiltrate with an IgG4 to IgG ratio of 1:4 and focally increased IgG4 plasma cells: 14 per high-powered field (see Figures 2A–D). Although obliterative phlebitis was not observed and the ratio of IgG4/IgG cells was not >40%, the overall histomorphological feature was suggestive of IgG4-related sialadenitis. The patient was started on prednisone, resulting in improvement of her submandibular swelling and arthralgias.
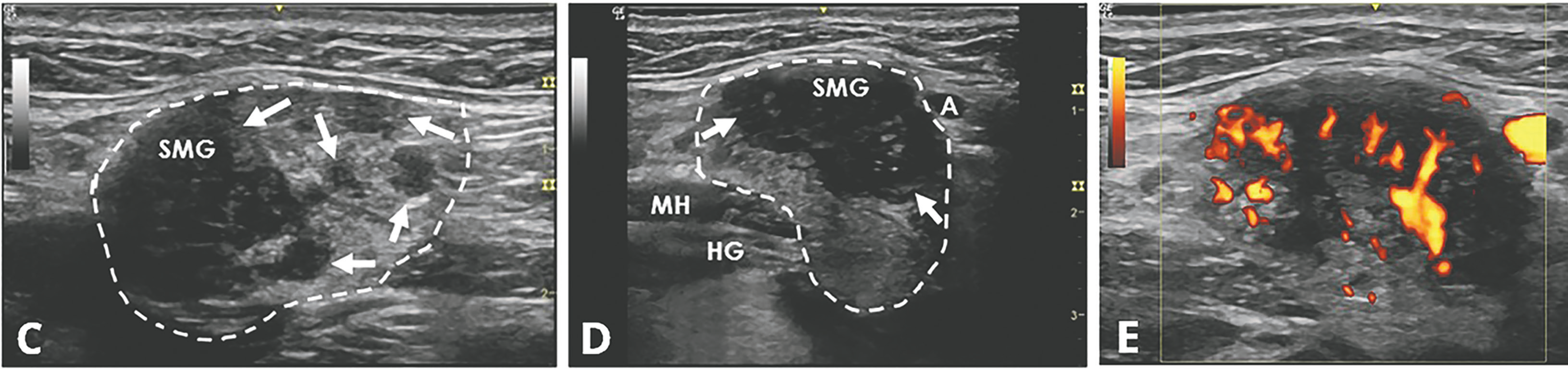
FIGURES 1 C, D & E: Left longitudinal submandibular gland with nodular hypoechoic lesions (C). Right longitudinal submandibular gland (D) with larger hypoechoic lesions producing a bulging on the surface of the gland. Large amount of Doppler signal within the right submandibular gland (E). Parotid gland (PG), submandibular gland (SMG), masseter muscle (M), mylohyoid muscle (MH) hyoglossus muscle, facial artery (A). The white arrows indicate areas of IgG4 involvement. The white dashed lines outline the glands. (Click to enlarge.)
Discussion
When a patient presents with submandibular gland swelling, xerostomia, xerophthalmia and positive anti-SSA antibody, Sjögren’s disease is usually at the top of the differential diagnosis. However, it is crucial to consider mimics of Sjögren’s disease, including IgG4-related disease (RD), lymphoma, sarcoidosis, amyloidosis, HIV-related and non-inflammatory causes (e.g., diabetes mellitus, alcoholism, liver cirrhosis and bulimia).