
FIGURE 1: Milk of urate bulla. (Click to enlarge.)
A 60-year-old Black woman with a history of stage 3 chronic kidney disease, type 2 diabetes and hypertension presented with a 12-month history of asymmetric polyarthritis of the wrists, metacarpophalangeal (MCP), proximal interphalangeal (PIP), metatarsophalangeal (MTP) and knee joints.
The review of systems was unremarkable. She denied oral ulcers, rashes, alopecia, or a history of pleural or pericardial effusions. She denied a history of psoriasis, dactylitis, inflammatory back pain, uveitis, abdominal pain, melena or hematochezia. There was no history of podagra, tophi or acute monoarthritis.
Arthrocentesis revealed inflammatory synovial fluid with 40,000 white blood cells/µL (neutrophil predominant). Gram stain, bacterial cultures and crystals were negative. She responded positively to glucocorticoids. Over the next year, her disease remained active in the hands, feet and knees, with minimal response to etanercept, tofacitinib or tocilizumab.
In October 2020, the patient returned to the clinic with hard, sub-centimeter, white lesions on her finger pads. A warm effusion of her left first MTP joint and a white blister on her left second toe were also noted on examination (see Figure 1). There was no sclerodactyly, Raynaud’s phenomenon or muscle weakness. Nailfold capillaries, muscle strength and creatinine kinase levels were normal.
Aspiration of the first MTP joint and blister yielded 5 cc of chalky white fluid (see Figure 2). Polarized light microscopy revealed negatively birefringent crystals consistent with monosodium urate. Her serum urate level was 9.7 mg/dL. Repeat radiographs of both hands and feet showed interval erosive changes in both midfeet, consistent with gouty arthropathy.
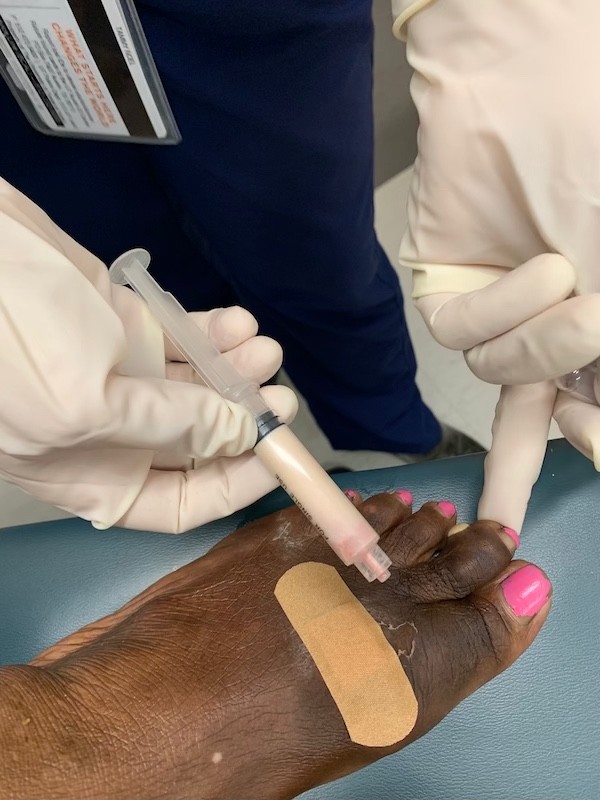
FIGURE 2: Milk of urate aspirated from the first MTP joint and milk of urate bulla. (Click to enlarge.)
Allopurinol was initiated and titrated to a goal serum urate of less than 6.0 mg/dL, per the 2020 ACR Guideline for the Management of Gout.1 Five milligrams of prednisone by mouth daily was continued as flare prophylaxis.


