click for large version
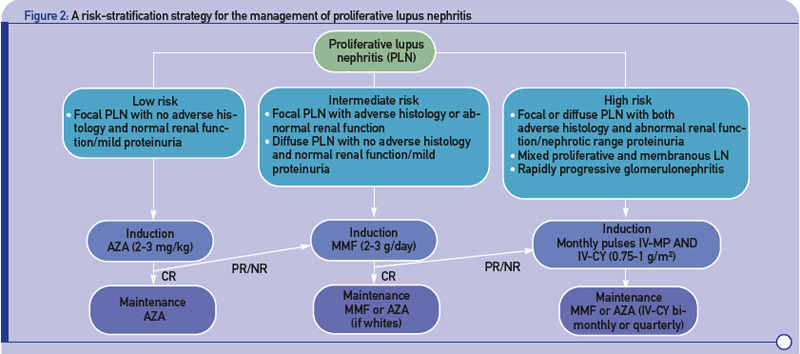
Figure 2: A risk-stratification strategy for the management of proliferative lupus nephritis.
- Stratification of risk for progression to end-stage renal disease based on findings of longitudinal observational studies, and retrospective analyses of RCTs or clinical cohorts. Adverse histology denotes the presence of crescents and/or fibrinoid necrosis affecting >25% of glomeruli; glomerular sclerosis, tubular atrophy, or chronicity index >4; or chronicity index >3 and activity index >10. Impaired renal function denotes increase in serum creatinine or reduction in estimated glomerular filtration rate (calculated by the Cockcroft-Gault or the Modification of Diet in Renal Disease formula) by >25%, or proteinuria >4 g/24 hr.
- Renal response is assessed at six months. CR is defined as decrease in proteinuria to <1 g/day (or <0.3 g/day in LN diagnosed in the past six months) with normal serum albumin concentrations; inactive urine sediment; and improved or stable renal function. PR is defined as significant change in proteinuria (if nephrotic at baseline ≥50% decrease in proteinuria to <3 g/day; if non-nephrotic at baseline but not meeting the CR criteria) and improved or stable renal function.
Abbreviations: CR, complete response; PR, partial response; NR, no response.
